By Dr Suzanne Humphries
Abbreviations:
SA sodium ascorbate
AA ascorbic acid
LSA liposomal/lipospheric sodium ascorbate
PSA powdered sodium ascorbate
WC Whooping cough
I wrote the original 2012 treatment document, based on Hilary Butler’s 30 years of research and my own experience and knowledge of toxin-mediated diseases.
My motivation to find a solution came from watching two young girls that were close to me, suffer from whooping cough. Neither conventional antibiotics nor homeopathic options helped at all. A skilled and revered homeopath was so concerned, that he even said to take the antibiotics. One girl refused and the other promptly vomited up her first dose and their mother was wise enough not to push the antibiotics. I later learned that there is little to no evidence that antibiotics help the severity or duration of cough in such children.
Both of those children recovered from an illness that neither will ever forget. Their excellent baseline health and nutrition no doubt helped them survive without any huge drama. Watching them cough, made me understand why anyone ever wanted to develop a vaccine against whooping cough. The problem is, the vaccine doesn’t work well at all and has toxicity issues. Had I known about the sodium ascorbate treatment, the girls would have had a much easier time of it.
A study of the medical literature showed that there was scientific rationale for such a treatment, which motivated me to start recommending vitamin C in those who have need, and to write the original document. After several years of expanded understanding of whooping cough in babies as young as 2 weeks of age, and older children, I’ve received hundreds of letters of appreciation telling me how the protocol worked for parents using it on their own.
Broader experience and observation have highlighted individual differences and unique situations, and resulted in technique refinements and improvements to the pre-existing write up. New medical literature references have also been added.
You must carefully read every word of this long document. Please do not jump to the protocol if you do not understand the full picture. If you do, you may struggle to work out how, when and why to adjust vitamin C dosing. Your child’s health and recovery is worth a few hours of your time to learn.
If you have a cooperative medical provider, this document can serve as a guideline for them and you to work together. However, as you will see by parents’ experiences on drsuzanne.net, most parents use the document on their own with success. Their stories will give you hope to put aside the negative messages propagated by ignorant and miseducated mainstream media and the conventional medical system.
B. pertussis infection as NOT a walk in the park. For many people it is a severe and worrying cough. If the B. pertussis vaccine was safe and effective, it may have been worth using. However, the B. pertussis vaccine is provably one of the most ineffective. It’s many disadvantages which lend dubious, fleeting protection to the individual, results in numerous doses and boosters from cradle to grave. In fact, the more whooping cough vaccines a person receives, the less effective they become.[1] Diavatopoulis has even compared the acellular vaccine that is used today, to allergy shots, because the cellular immune system responds less and less after successive doses in those who have been primed with acellular vaccines.
Conversely one episode of natural whooping cough renders the recovered person immune far longer than any series of vaccines will.
The information provided here is distilled from a wide body of literature that demonstrates that the ascorbate molecule, in frequent doses, is extremely safe. Experience shows it to be instrumental in the biochemical recovery from Bordetella pertussis (whooping cough) infection. Natural recovery from whooping cough has advantages for an entire life.
Bordetella pertussis infection
While it is not ideal for a newborn infant to catch whooping cough, it can be managed at home. Successful treatment will require diligence and an adult rocking very young infants, at the peak of infection, 24 hours for several days. Babies cannot get vaccinated until they are two months of age, and by then, the cough can be treated much more easily than in a younger infant. After three months, a fully breast-fed baby will respond well. Otherwise healthy babies over six months of age with whooping cough, should not worry any parent if they understand the principles and protocols to deal with the infection, and are well equipped and organized.
B.pertussis bacteria is very tricky, and part of its armor involves several toxins. Toxin production is the major reason for the worst symptoms. Conventional medical doctors don’t know how to address the toxin issue in most infections. They give antibiotics, which have never been shown with any certainty, to limit the duration or severity of whooping cough in well-established disease.
After years of experience treating infants of all ages, it has become evident that there are some exceptions to the antibiotic issue:
- In 2 week to 2 month age babies, if the antibiotic is given at the first sign of cough, the severity of cough can often be decreased. I’ve worked that out with observation and use, but the two doses of antibiotic have to be given at the very first signs of the first phase of the illness. This can only happen if the index case has previously been identified and the parents know what is coming.
- This does not seem to be the case in older babies, where parents almost always report worsening symptoms after the antibiotic has been given. This may be due to starting them after the cough is full blown. I’ve not tried the two days treatment with azithromycin on older babies, because IMO, the risk:benefit is not there at that age. One exception could be someone with cystic fibrosis or other underling lung problems. But again, it will probably only make a difference if the cough is anticipated as a result of knowing that the exposure occurred.
- Antibiotics don’t seem to help whooping cough symptoms in anyone at any age, after it has become a full blown infection.
Is ascorbate a cure? No, but the majority of parents who use it on their infected babies, and young and older children, report a significant decrease in cough intensity, with thinning and loosening of sticky mucus, within the first 24 hours of proper dosing. Ascorbate, in properly spaced, very high oral doses, will get you and your children through the weeks with vastly reduced symptoms while developing lasting immunity that will later protect those around them more effectively than vaccines can.
A 2010 study suggested that natural immunity to whooping cough lasts at least 30 years[2], whereas the immunity from a vaccine lasts three years at most.[3]
Because of the limited duration of transient immunity after vaccination, B. pertussis boosters are now being recommended for 8-12 year-olds, adults, women during each pregnancy, and contacts of newborns before every birth.
If you think that a vaccinated person cannot get whooping cough, in the most severe manner, think again. Most babies over the age of 6 months who get whooping cough are fully and “appropriately” vaccinated. In 2012, a new peer reviewed document from professor of infectious diseases, Dr Maxwell Witt of Keyser Permanente in California showed that B. pertussis runs rampant in fully vaccinated child populations.
“Our data suggests that the current schedule of acellular pertussis vaccine doses is insufficient to prevent outbreaks of pertussis. We noted a markedly increased rate of disease from age 8 through 12 . . . . Acellular vaccines have not been studied for clinical efficacy in north America and no studies exist on long term.”[4]
Quite impressive, right? Table 1 at the end of Dr Witt’s document shows the percent of cases in the vaccinated, and it as follows: 86% age 2-7, 86% age 8-12, 62% age 13-18, 81% age 2-18. So now you know who gets more B. pertussis. It is not the unvaccinated. He even says, in the introduction:
“Our unvaccinated and under-vaccinated population did not appear to contribute significantly to the increased rate of clinical pertussis. Surprisingly, the highest incidence of disease was among previously vaccinated children in the eight to twelve year age group.”
The rate of infections in the vaccinated is huge. Look at this chart prepared by the California Department of Public Health, Immunization Branch.
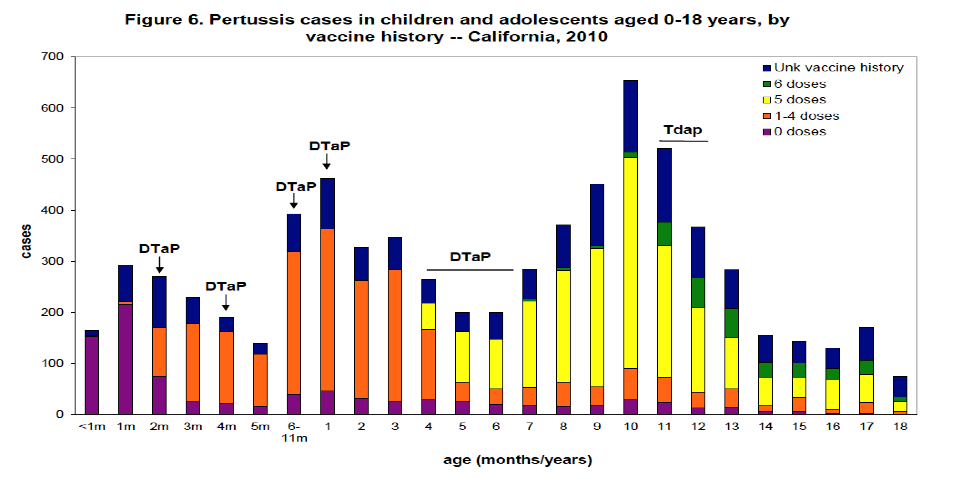
The above chart was last printed in the California department of public health pertussis report[5], November 10, 2011. Thereafter, the report on cases by vaccine history stopped. In fact, word searching for ‘vaccine’ brings up no data in the recent reports. It just says to give the vaccine in infancy and pregnancy.
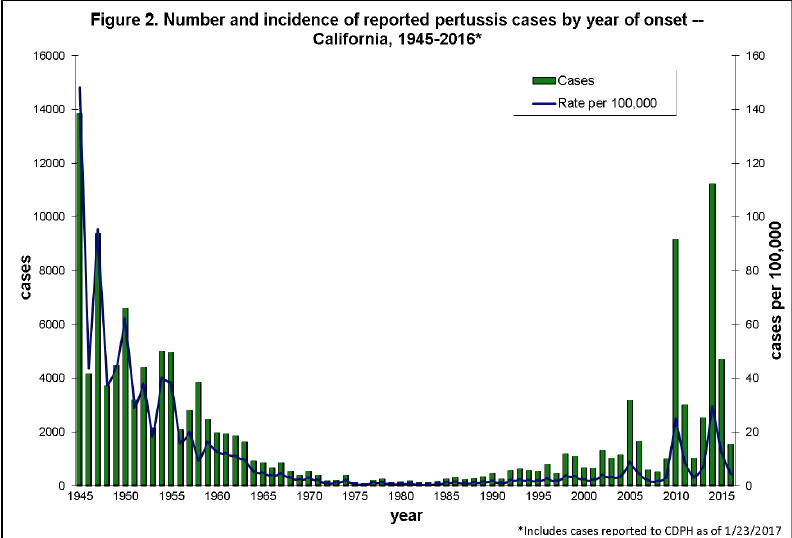
Graph above from
https://archive.cdph.ca.gov/programs/immunize/Documents/pertussis_report_2017-1-23.pdf
Vaccine defenders will say that the high rate in the vaccinated is just because the majority of people in the population are vaccinated There are known and published reasons why vaccinated children are becoming infected, even at high vaccine compliance rates which I have discussed elsewhere.
See my herd immunity lectures here https://www.youtube.com/playlist?list=PLgH2vCx5TOgXZrRRM-ObX7JXt_0Ie8OI0&disable_polymer=true
The fact is, that regardless of whether a child is vaccinated or not, everyone needs to be able and ready to treat whooping cough.
Personal protection: Who wins out?
Vaccinated babies, children, and adults are not able to mount the comprehensive bronchial and cellular immunity that a non-vaccinated person naturally develops in the course of the disease.[6] Why? Because the vaccine primes the body to fight B. pertussis toxin and sometimes a couple of other bacterial antigens, in the blood, but does not provide protection at the lung interface where the real-life battle occurs. The ineffective immunity “learned” from the vaccine series (referred to by Dr. James Cherry as “original antigenic sin”)[7], is the same way the body will respond to a subsequent natural exposure.
The learned immune response to an acellular vaccine results in numerous differences compared with the normal response mounted to a natural infection. Some of the key differences in vaccinated people are:
- Antibody preferentially made in the blood rather than the lung interface.
- IgG antibody rather than IgA antibody.
- A relatively different and ineffective antibody because the vaccine antigens are not the same shape as the real life antigens.[8]
- A relative, progressive loss of protection with each vaccine dose, because the T cell response is similar to what allergy injections do.[9]
- Far lower complement-mediated killing of bacteria.
- Suboptimal inflammatory responses resulting in impaired lung clearance of bacteria.
- Impaired phagocytosis.
It is well known that never-vaccinated B. pertussis disease-convalesced children, develop important immune responses that the vaccinated do not[10]. Vaccine developers have attempted to compensate for this phenomenon by creating vaccines with multiple antigens. The point they miss, is that it is only front line, innate, and naturally acquired complex-cellular and bronchial responses, which give the full protection. It has been shown that response to B. pertussis toxin[11] and adenylate cyclase toxin[12] is far more robust in the unvaccinated, than the vaccinated. Because of this, naturally immune people, upon re-exposure, will clear bacteria far more rapidly than the vaccinated will. There is an enormous difference between broad, long-lasting immunity from the normal disease, and limited antibody development and short-term pseudo-immunity from the vaccine.
If your child has whooping cough, the doctor will try to make you give antibiotics even though antibiotics do not shorten the sickness, or do anything to lessen the seerity of the disease once the cough is full blown[13]. But often, even alternative doctors will suggest antibiotics because they don’t know the medical literature and because they want to just DO something. The conventional medical culture does not seem to understand the damage created by unscrupulous use of antibiotics.
Antibiotics given during full-blown infection seem to make the sickness worse in most people. They can actually make the coughing fits more severe by releasing LPS(lipopolysaccharide) from other gram-negative gut bacteria during the microbial die-off that happens.
[…]
Click this link for the original source of this article.
Author: stuartbramhall
This content is courtesy of, and owned and copyrighted by, https://stuartbramhall.wordpress.com and its author. This content is made available by use of the public RSS feed offered by the host site and is used for educational purposes only. If you are the author or represent the host site and would like this content removed now and in the future, please contact USSANews.com using the email address in the Contact page found in the website menu.



