In my opinion, the paper below is one of the most significant papers in the field of Pediatrics in modern times. Published in 2021, it should have been heralded as a landmark paper in public health, and its findings should have been widely disseminated.
In this dream world of mine, that paper would have been published in Pediatrics, the flagship journal of the American Academy of Pediatrics (AAP). In such a non-pharma-controlled world, its findings would have then been immediately broadcast via the media (TV, radio, newspapers, etc.). If non-conflicted science journalism and talk shows still existed, this would have led to an extended round of interviews on the media circuit with the author, Niel Miller.
I would argue this would have, finally, exposed to all American parents the hitherto suppressed and unacknowledged lethal risks of vaccination in infants.
OK, sorry, I got carried away there. Of course, that wouldn’t happen because those actions would have instead resulted in an epidemic of the most feared disease of our Public Health establishment, that of “vaccine hesitancy” in our nation’s mothers and fathers.
Unsurprisingly, the paper was instead published in a peripheral journal called “Toxicology Reports.” In that field, it is reasonably well regarded, but who reads toxicology journals? At least it was in a decent peer-reviewed journal, so all hope is not lost.
The following review, which examines the data supporting the association between vaccination and skyrocketing infant death rates over the last 60 years, was heavily (but not entirely) informed by the Miller paper above, its extensive bibliography, and this excellent review of the topic by my friend and colleague, A Midwestern Doctor.
SIDS – Sudden Infant Death Syndrome
In 1969, for the first time in history, at the International Conference on Causes of Sudden Death in Infants, the National Institute of Child Health and Human Development coined the term SIDS and defined it as:
“The sudden death of an infant under one year of age which remains unexplained after a thorough case investigation, including performance of a complete autopsy, examination of the death scene, and review of the clinical history.”
In Miller’s 2021 paper, which reviews patterns of deaths reported to VAERS, he conducted a review of both epidemiologic data and published studies that have explored the temporal relationships between vaccine administration and unexplained infant deaths. I will start with just one of the many “truth bombs” it contains:
Before widespread vaccination in the 1960s, “crib death” was rarely reported. After new vaccines were introduced and immunization campaigns expanded, sudden infant death syndrome (SIDS) emerged as a recognized cause of death. It became the leading cause of post-neonatal mortality in the U.S. by 1972.
The reference above was from this aptly sub-titled book:
So, SIDS went from virtually non-existent to the #1 cause of infant death in a less than 20-year period. Hmm. The problem I had with the statement above is that it was not referenced. So I turned to AI to find data to support it.
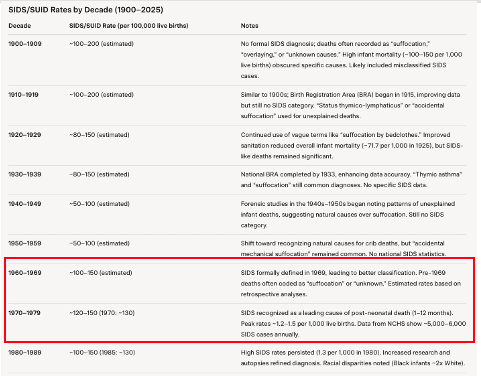
See this below table of rates of unexpected infant deaths that it generated – why, after steadily decreasing from the turn of last century, did unexpected/ suffocation/strangulation deaths suddenly double between the 1950’s and 1960’s and then almost triple in the 1970’s compared to the 1950’s (and remained newly historically high in the 1980’s)?
If better sanitation, hygiene, pre-natal care, medicine, and health care was steadily improving during the 20th century as reflected in steadily decreasing rates of these types of infant deaths, why, suddenly, in the 1960’s, did infants started dying at rates similar to those being born in the early 1900’s? Why were we suddenly moving backwards in time?
Then, throughout the 1980s, sudden infant deaths continued to remain elevated. Parental concerns about an apparent link between childhood vaccines and SIDS rose rapidly, and Pharma’s #1 enemy, that of “vaccine hesitancy,” began to permeate society, with many parents becoming afraid to vaccinate their babies. Oh no!
The above concerns spreading amongst the general public were compounded by media coverage, such as the 1982 documentary “DPT: Vaccine Roulette.” Some argue this was the last major media exposé of the harms of vaccines, although that would overlook the three talk shows that Phil Donahue did in 1983, 1986, and 1990. Since then, almost nothing in corporate media. Note, I could find no links to the videos of the Phil Donahue shows on the internet, but AMD posted a recording of the 1986 episode in this post.
Many parents with DPT-injured children saw the documentary, called NBC, and then were connected by NBC, forming “Dissatisfied Parents Together,” one of the original vaccine safety groups, and in 1985, a book called DPT: A Shot in the Dark was published.
•As early as 1933, there were published reports of infant deaths shortly after DPT shots, including some where autopsies attributed the deaths to vaccination.
•Simultaneous identical twin deaths are an extraordinarily rare event and are hence considered a gold standard for establishing causality. In 1946, two twins died (on their backs) within 24 hours of their second DPT vaccine— something also shown in 1987,2006, 2007,2010, and 2013 case reports.
•Researchers like Dr. William Torch (who analyzed 72 sequential SIDS cases and then over 200) showed that these deaths clustered shortly after vaccination, something which could not be explained by chance.
Then, in 1984, likely in response to public outcry, Congress held a hearing on vaccine safety. The suspected link between vaccines and sudden infant deaths was addressed. The following excerpt is from a statement made by a distraught grandmother testifying before the Congressional Committee (the original reference to this hearing from Miller’s paper was from Elsevier and can no longer be found (even on Wayback machine – shocker), nor can I find it in government archives – pre-digital era I suppose):
My name is Donna Gary. Our granddaughter, Lee Ann, was just 8 weeks old when her mother took her to the doctor for her routine checkup. That included her first DPT inoculation and oral polio vaccine. In all her entire 8 weeks of life, this lovable, extremely alert baby had never produced such a blood-curdling scream as she did at the moment the shot was given. (Ed: Infants do have a “voice” (they scream); it is just that no one understands the significance.) Neither had her mother ever before seen her back arch as it did while she screamed. She was inconsolable. Four hours later, Lee Ann was dead. “Crib death,” the doctor said—”SIDS.” “Could it be connected to the shot?” her parents implored. “No.” “But she just had her first DPT shot this afternoon. Could there possibly be any connection to it?” “No, no connection at all,” the emergency room doctor said definitely. Are the statistics that the medical world loves to say, “There is no connection,” really accurate, or are they based on poor diagnoses and poor record keeping? What is being done to provide a safer vaccine? How will physicians and clinics be held accountable to ensure that parents are informed of the possible reactions? And how are those children who should not receive the vaccine to be identified before they are damaged or dead?
Things were really starting to go sideways for the vaccination industry here. So what did Pharma do? Well, in 1994, they got the Institute of Medicine (IOM) to publish a report in response to public concern:
It is my opinion, that, like many studies published in response to “science that is inconvenient to industry,” the above report is a classic example of the Disinformation tactic called “the Fake” from the “Disinformation Playbook” by the Union of Concerned Scientists, i.e. the report was written with a pre-determined goal: to discredit the notion that there was causality between vaccines and newly exploding rates of infant deaths.
Recall the definition of “The Fake” from that article:
The IOM report is a clown show of a document – they examined the death reports associated with each vaccine on the schedule and repeatedly reached the same conclusions: 1) that there was not enough data to establish causation, and 2) that “more aggressive tracking and follow-up should be performed.”
Notably, it was around this time that the Vaccine Adverse Event Reporting System (VAERS) was created. VAERS is a national safety surveillance program that collects information about possible adverse reactions to vaccines. It should come as no surprise that, as per Miller:
“Public health authorities have never conducted the type of comprehensive investigation that is required to definitively prove or disprove a causal relationship between vaccines and SIDS. VAERS data, which is the only publicly available post-marketing adverse event database in the U.S., has been largely ignored or dismissed when it suggests a link between vaccination and sudden infant death.”
Coincident with the IOM report in 1994, the CDC and the American Academy of Pediatrics began a campaign to reassure parents that sudden unexplained infant deaths (SUID) following vaccination were coincidental and not causally linked to vaccines.
I want to state the obvious here – it is clear to me that the primary objective of these agencies was to combat vaccine hesitancy and NOT to ensure safe vaccines (there is no such thing, because we know that the main argument given by Pharma executives in support of the National Childhood Vaccine Injury Act of 1986 (which then severely limited their liability exposure) was that vaccines were “unavoidably unsafe.” I maintain that since then, a major objective of our public health agencies has been to “gaslight” the American public every time a healthy child (or clusters of them) die within hours or days of a vaccine or vaccines.
What is weird is that indoctrinated pediatricians, propagandized from Day 1 of medical school, do this for them – any parental concerns are dismissed or refuted, like in the Congressional testimony above.
Click the first AAP link below to see the list of lies they have been propagating since that time:
CDC helped spread the message too:
In the AAP document, these gems appear:
In the last 15-20 years, as our scientific understanding improved, medical experts realized that a proportion of sudden deaths were caused by suffocation rather than an unknown cause. Therefore, the term was expanded to SUID.
Sudden Unexpected Infant Death, or SUID, is an umbrella term that covers accidental suffocation and strangulation in bed, SIDS, and other deaths from unknown causes.
Problem: Although they somehow could not find an association of the explosion in sudden, unexpected infant deaths with the advent of vaccination programs in the 1960s, nowhere did they explain why infants, after being born for millennia, were suddenly “suffocating and strangulating” themselves in bed.
The AAP’s “Back To Sleep” Campaign
What was the U.S. public health response to this sudden public health emergency? The AAP’s “Back to Sleep Campaign” in 1992:
The above “policy recommendation” by the august AAP led pediatricians all over the country to start recommending to parents that they place their infants on their back to go to sleep so they would not strangle or suffocate themselves (it is hard to write that with a straight face). Please forgive me for overusing the term “clown world,” but, on this topic, I will be forced to do so repeatedly, so here goes: Clown. World.
I find it odd that since humans started roaming the Earth and civilizations began to flourish, producing insights and achievements one more remarkable than the other, that the Greeks, Romans, Incas, Persians, Mayans, British, Indians, Chinese etc (sorry if I am leaving some out), never figured out that infants should be placed on their back to go to sleep to avoid “strangulation in bed.” It was not until an AAP committee in the early 1990s figured out that by placing infants to sleep on their backs, this scourge could be stopped. Wow. Modern public health at its absolute finest.
Now, to be fair, there were several (small) studies published at the time which suggested that SIDS infants were found more often in the prone position, so it may not have been as clownish as I first maintained above. I will address this below.
However, I need to point out the fact that most infants can sleep however the $%&! they want. From developmental guidelines: “Infants start rolling from their stomach to their back around 4-5 months and from their back to their stomach around 5-7 months.” Yeah, “Back to Sleep,” that’ll work.
Guess what? It did! I am such a fool. Perhaps those studies were correct! Incredibly, the post-neonatal SIDS rate dropped by an average annual rate of 8.6 % from 1992 through 2001. Wow! Thank God for the astute clinicians and researchers who devised such a brilliant public policy intervention. Who woulda thunk it?
Problem: The post-neonatal mortality rate from “suffocation in bed” (ICD-9 code E913.0) increasedduring this same period at an average annual rate of 11.2 %. Uh oh.
From the Miller paper:
The post-neonatal mortality rate from “suffocation other” (ICD-9 codes E913.1-E913.9), from “unknown and unspecified causes” (ICD-9 code 799.9), and from “intent unknown” (ICD-9 codes E980-E989), all increased during this period as well [9]. In Australia, a similar subterfuge seemed to occur. Researchers observed that when the SIDS rate decreased, deaths attributed to asphyxia increased.
Basically, what happened was that coroners started pulling a “bait and switch” by classifying infant deaths using other classification codes than SIDS, which reassuringly led “SIDS” rates to drop. Although I don’t know the answer, I wonder just how they were influenced to start changing their classifications of infant deaths? Cash payments? Policy recommendation from the International Association of Coroners & Medical Examiners (IACME)? I made Grok AI try hard, but it could find no documents or specific classification policy recommendations from that time from the IACME or the CDC. Scrubbed from the internet or hidden in pre-digital archives?
More ICD Coding Shenanigans
Another move they made to more definitively rule out the association, err, I mean causation between vaccination and death is that, get this, when the ICD was revised in 1979—and in all subsequent updates to the ICD—all cause-of-death classifications directly associated with vaccination were eliminated. Although Miller stated the above in his review, I could not find a reference for it, so I asked Grok – I was given a link to this article from The Liberty Beacon:
From SIDS to SADS: how the pharmaceutical-industrial complex fiddles the stats to hide its killings. June 11, 2022.
Problem, although Grok provided the link to the article, when I clicked on it, I got this, shocker:
I asked Grok for other supporting documentation for the decision to remove this disturbing classification code, and this is what it came up with:
ICD-8 (1968–1978): Included E934 for deaths due to “prophylactic inoculation and vaccination,” allowing medical certifiers to attribute deaths directly to vaccines or biological substances. This code was part of the external causes of injury section (E800–E999), reflecting adverse effects of medical interventions.
ICD-9 (1979–1998): Removed E934, replacing it with broader codes like E928.3 (other preventive measures) or E949 (other vaccines and biological substances). These codes are used for complications or adverse effects, but are not specific to death as the primary outcome. For example, a vaccine-related anaphylactic death might be coded as T78.2 (anaphylactic shock) with E949 as a secondary code, but the vaccine itself is not listed as the underlying cause.
Unreal. They covertly removed it from the ICD without publicly acknowledging the change, leaving the only way to discover it by carefully looking at the presence or absence of vaccination death codes between ICD revisions. Strong work, Pharma.
Infant Deaths Remain Elevated
Anyway, the bait and switch worked for a while.. until 1999, when it was discovered that:
From 1999 through 2001, the number of U.S. deaths attributed to “suffocation in bed” and “unknown causes” increased significantly. Although the post-neonatal SIDS rate continued to decline, there was no significant change in the total post-neonatal mortality rate.
Then the data really started to go sideways:
From 1999 through 2015, the U.S. SIDS rate declined 35.8 % while infant deaths due to accidental suffocation increased 183.8 %.
Now, to be fair, although all the above is true, my ridicule of the efficacy of “Back to Sleep” programs is somewhat undeserved. In my review of the data since, I have to admit that subsequent overall infant mortality decreases can be partly attributed to such campaigns, but nowhere near the magnitude that Public Health authorities initially claimed as above.
How Japan Responded To Vaccine-Induced Infant Deaths
Let’s contrast the above series of actions by U.S Public Health Agencies and academia with what Japan did in response to the same epidemic of infant deaths (which they noticed almost 20 years prior). From the Miller review:
In Japan, from 1970 through 1974, there were 37 documented sudden infant deaths following pertussis vaccinations, inciting parents and doctors to reject the shot. In 1975, Japanese authorities reacted to these events by raising the age of vaccination from 3 months to 2 years. As a result, the number of vaccine injury compensation claims that were paid out for sudden deaths following vaccination dropped from 37 cases during a 5-year period to just 3 cases during the next 6-and-a-half years (from 1975 through August of 1981).
The sudden death rate following vaccination dropped from 1.47 to 0.15 deaths per million doses—a 90 % improvement [40,41]. In addition, from the early 1970s (a period when 3-month-old infants were vaccinated) to the mid-1980s (ten years after the age of vaccination was raised to 2 years) the Japanese infant mortality rate (infant deaths per 1000 live births) declined from 12.4 to 5.0—a 60 % improvement [42]. A special Task Force on Pertussis and Pertussis Immunization investigated the Japanese data and published their report in the journal Pediatrics. According to Cherry et al. [41], “The category ’sudden death’ is instructive in that it disappeared following both whole-cell and acellular vaccines when immunization was delayed until a child was 24 months of age.” The special Task Force also made the following observation: “It is clear that delaying the initial vaccination until a child is 24 months, regardless of the type of vaccine, reduces most of the temporally associated severe adverse reactions.”
Whoa. How is that for a public health intervention? I can’t believe they achieved that reduction without chastising Japanese mothers to put their infants to sleep on their backs! Sorry, I just can’t let that one go (but again, to be fair, several decades later, “Back to Sleep” recommendations began to proliferate in Japan and do appear to have led to even further reductions).
Further evidence that delaying vaccination in infants reduces their risk of dying can be found in U.S data as well. Back in 2012, Goldman and Miller (yes, the same Miller) published an analysis of 38,000 infant reports filed with VAERS. The hospitalization rate for infants vaccinated shortly after birth was an astonishing 20.1%, but decreased in a statistically significant linear fashion to 10.7% for infants vaccinated just before their first birthday. The same decrease was observed regarding infant deaths.
Maybe, just maybe, we are vaccinating babies at too young an age? Except for Hepatitis B, of course – that one is critical to be given on the first day of life because of the large cohort of infants that crawl out of maternity wards to hit the streets, injecting drugs and having sex with prostitutes (sorry, I just can’t help myself here).
If you find value in the time, research, and care I invest in crafting these posts to expose critically important truths about the safety and efficacy of a diverse set of medical therapeutics, please support my work with a paid subscription.
VAERS Analyses Revealing Tight Temporal Associations Between Vaccination And Death
The title above is the crux of the Miller paper (and was briefly covered in my recent post on the twin deaths in Idaho) but I will go into more depth here, and will ask my regular readers to forgive me for any redundancy.
What Miller did was review all reports of SIDS and/or infant deaths to VAERS over 20 years, from 1999 – 2019 (i.e., SIDS deaths suspected to be related to vaccination). He then analyzed the frequency of deaths according to the days post-vaccination. He hypothesized that, if vaccines did not cause deaths, then the number of fatalities reported would be evenly distributed on each day after vaccination, i.e., the number of fatalities one day post-vaccination would be the same as 11 days, 21 days, and 35 days, etc.
What did he find instead? You guessed it:
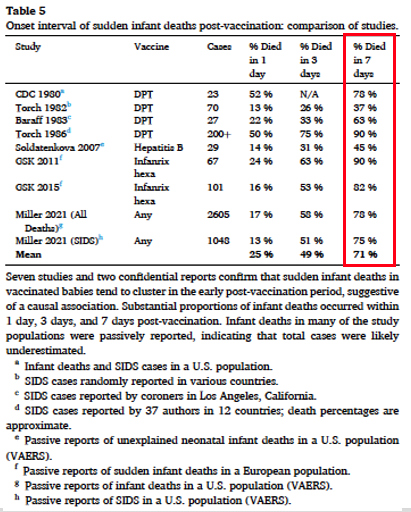
Of the 2605 infant deaths, 58 % clustered within 3 days post-vaccination and 78.3% within 7 days post-vaccination.
Of the 1048 SIDS cases, 51 % clustered within 3 days post-vaccination and 75.5 % within 7 days post-vaccination
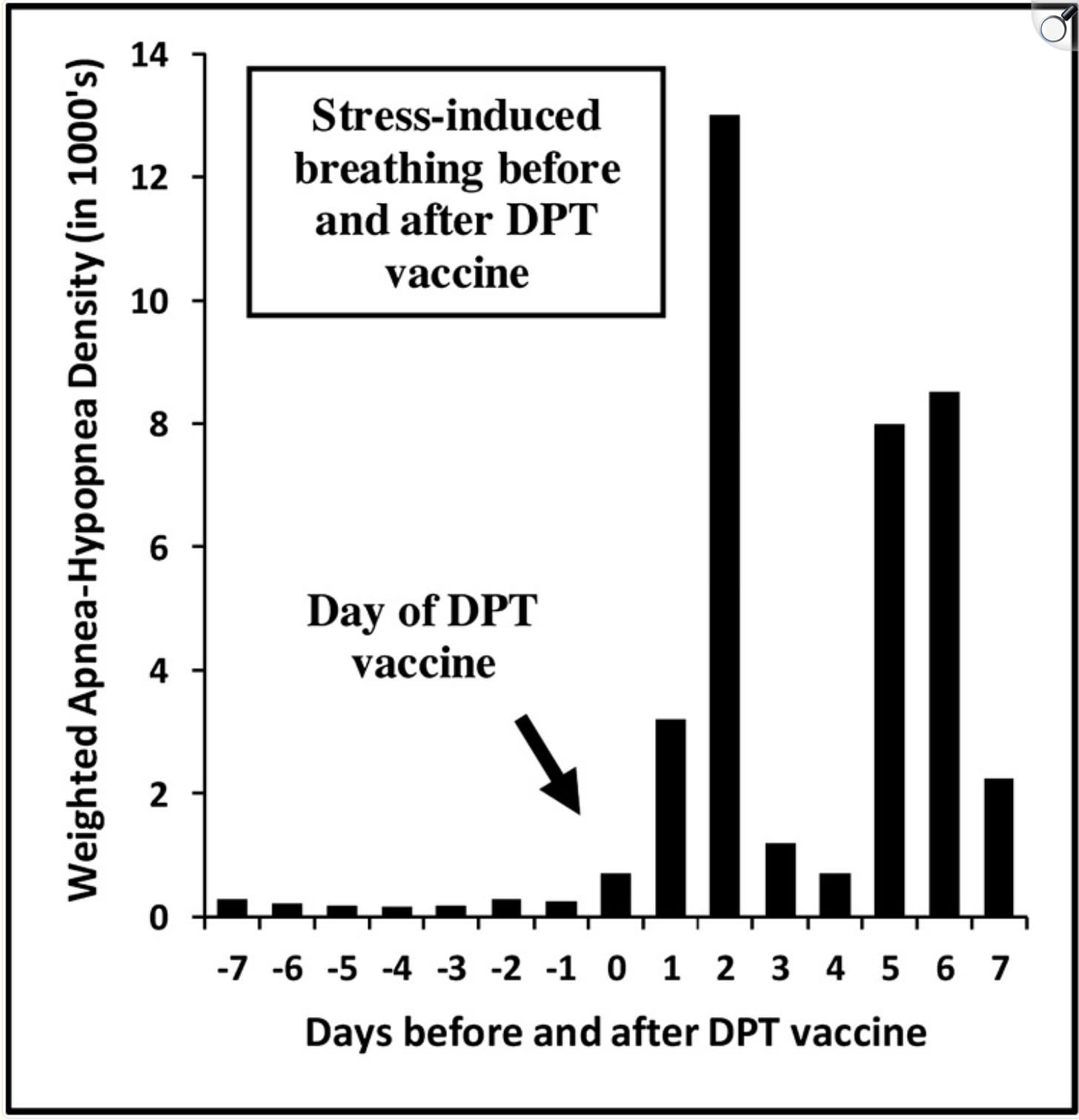
Again, as I briefly reviewed in my recent post, the above distributions of deaths shockingly mirror the frequency and distribution of post-vaccination apneas (episodes of cessation of breathing) and hypopneas (shallow or slowed breathing), as depicted below, reported by Schreibner et al. In that study, they placed a sophisticated microprocessor under the mattresses of infants to precisely measure their breathing patterns before and after pertussis vaccination. Note that the y-axis measures these episodes in the thousands.
From Miller: “The data revealed that pertussis vaccination caused an inordinate increase in episodes where breathing either nearly ceased or stopped completely.”
One of the most damning and disturbing aspects of the data presented above is the frequency of apneas in the days leading up to vaccination – minimal and unvarying, setting a stable, inconsequential background rate. Then, suddenly, vaccination occurs, and there is an approximate tripling of the apnea/hypopnea rate on that day. However, this is nothing compared to 2 days after vaccination, when the rate literally explodes (approximately 50 times), only to rapidly decrease and then increase again on days 5-7. Although the graph above ends on Day 7, the study found that these episodes continued for several months post-vaccination before returning to baseline.
Let’s take Miller for what it is – basically, all kids were vaccinated (they were in VAERS) and he looked for a temporal association with the vaccine. The vast majority died within a week, when, again, if these deaths were random and unassociated, you would expect the same # of deaths each day for weeks after the vaccine, yet 70% occurred within a week.
Have others found similar? Yes, yes, yes, and yes:
In 1980, analyses of additional data collected by the CDC revealed 23 deaths within 28 days following DPT vaccination, 52.2 % occurred within 24 h, and 78.3 % occurred within 1 week.
In 1983, Baraff et al. reported on 27 infants; a statistically significant number of excess deaths happened during the first week post-vaccination. According to the lead author, “This study further substantiates the possible association between DTP immunization and SIDS.”
In 1986, Torch et al. summarized case reports of more than 200 deaths that occurred following DPT vaccination, as reported by 37 authors in 12 countries. About half of these deaths occurred within 24 h, 75 % within 3 days, and 90 % within 1 week post-vaccination.
In 1987, Walker and colleagues found that babies died at a rate more than 7 times greater than expected in the period 0–3 days following DPT vaccination when compared to the period beginning 30 days post-vaccination.
In 1982, a study at the 34th Annual Meeting of the AAP reported on 70 cases of deaths after DPT. 66% had been immunized within 21 days before death. 6.5 % died within 12 h of inoculation, 13 % within 24 hours.
** The above study reported that unvaccinated babies who died from SIDS did so most often in the fall or winter. In contrast, vaccinated babies died most often at 2 and 4 months, the same ages when initial doses of DPT were given to infants.
The author concluded (back in 1982!) that…“DPT may be a generally unrecognized major cause of sudden infant and early childhood death, and the risks of immunization may outweigh its potential benefits.” Ya don’t say.
Full disclose and transparency here: I came across a blistering critique and rebuttal of the Miller paper by the most famous troll of vaccine skeptics (and troll of all alternative medicine which he labels “pseudoscience”), the one and only Dr. David Gorski (who, humorously has dubbed my esteemed and erudite colleague AMD, “A Midwestern Quack”).
Gorski has gone after me and my ivermectin “pseudoscience numerous times on social media and in blog posts. I find him amusing in his consistent antagonism for anything that deviates from Establishment narratives. Most revealing about him (and people like Peter Hotez) is his repeated refusal to debate any vaccine skeptic, such as Dr. Sheri Tenpenny or RFK Jr. (the two of them would likely wipe the floor with him, and he knows it). It was a very weak, largely ad-hominem critique and was easily rebutted by Goldman and Miller. Can read the full article posted by the Liberty Beacon here but I will briefly excerpt it below.
Gorski’s Critique of the Miller-Goldman Study
Gorski argued that Goldman and Miller had conflicts of interest that swayed their analysis — Miller, because he operates a website that promotes informed consent, and Goldman, because he founded a medical journal that published papers critical of vaccines. Strong work, Dr. Gorski.
“What Gorski failed to mention is that Goldman is an expert on the varicella virus and for eight years worked as an epidemiology analyst for the CDC in collaboration with the Los Angeles County Department of Health … to help conduct epidemiological studies of varicella disease at one of the three surveillance sites …
Goldman vaccinated his own children and supported vaccination at the population level during his tenure with the CDC. Goldman has also served as a professional peer-reviewer for numerous medical science journals …” Miller wrote in a rebuttal to Gorski’s review.
Goldman had initially joined the CDC, thinking that it was the gold standard in unbiased research, but over the years, he realized that wasn’t the case. The CDC barred him from publishing any findings that linked the vaccination program with negative health outcomes, which led to his resignation in 2002, as he did not want to participate in research fraud.
He discussed the CDC’s suppression of undesirable vaccine data in a January 2022 interview. Then, all of a sudden, in December 2022, members of the Miller Lab at Brigham Young University in Utah, as part of the BYU Bioinformatics Capstone course, reanalyzed the Miller-Goldman paper and tried to debunk it yet again.
The critique, posted on the preprint server medRxiv (which is still not peer-reviewed), claimed Miller and Goldman had employed “inappropriate data exclusions” to reach their conclusion, as they didn’t analyze the full dataset, which included 185 nations.
“We re-analyzed the original data used in Miller and Goldman’s study to investigate the relationship between vaccine doses and IMR,” the authors write.
“We show that the sub-sample of 30 countries used in the original paper was an unlikely random sample from the entire dataset, as the correlation coefficient of 0.49 reported in that study would only arise about 1 in 100,000 times from random sampling.
If we investigate only countries with high or very high development, human development index explains the variability in IMR, and vaccine dose number does not.
Next, we show IMR as a function of countries’ actual vaccination rates, rather than vaccination schedule, and show a strong negative correlation between vaccination rates and IMR … From our analyses, it is clear that vaccination does not predict higher IMR as previously reported.”
“The critics’ reanalysis combines 185 developed and Third World nations that have varying rates of vaccination and socioeconomic disparities. Despite the presence of inherent confounding variables, a small, statistically significant positive correlation of r = 0.16 (p < .03) is reported that corroborates the positive trend in our study.
ED: For brevity, I left out the sophisticated summary of their statistical analyses and will end with their conclusion:
Conclusions: A positive correlation between the number of vaccine doses and IMRs is detectable in the most highly developed nations but attenuated in the background noise of nations with heterogeneous socioeconomic variables that contribute to high rates of infant mortality, such as malnutrition, poverty, and substandard health care.”
There you have it. As the Liberty Beacon article stated,
“Through the years, the Miller-Goldman paper has often been cited as evidence that the U.S. childhood vaccination schedule may be doing more harm than good. And, aside from an early debunking attempt by Dr. David Gorski, a surgical oncologist, the paper has stood the test of time.”
Pertussis Vaccines Are Used To Induce Brain Injury In Animal Studies Experimentally?
This was absolutely shocking to learn for me. From the Schreibner apnea study above:
Vaccines, such as pertussis, have been used in animal studies to induce “experimental allergic encephalomyelitis” (Levine et al, 1966; Levine and Sowinski, 1979; Steinman et al, 1982; and many others).
Steinman et al (1982) vaccinated mice with the heat-killed Bordetella pertussis vaccine combined with bovine serum albumin (BSA). They concluded that neuropathology in their mouse model resembles that of human cases in which death has occurred after DPT vaccination: diffuse vascular congestion and parenchymal haemorrhage in both the cortex and white matter. Cortical neurons showed ischemic changes, and areas of hypercellularity were evident in the meninges. B. pertussis has a wide range of physiological effects, including increased IgE production, increased sensitivity to anaphylactic shock, lymphocytosis, and hyperinsulinemia. Its ability to induce increased vascular permeability may account for the tendency to produce haemorrhages. The relevance of the murine model of pertussis vaccine encephalopathy is demonstrated by most babies being exposed to cow’s milk (even in breast-fed babies) due to pre-existing anti-BSA antibody. This sensitisation to BSA may lead to a similar chain of events following pertussis vaccination in genetically susceptible human babies
Bonilla and Oettgen (1997) analyzed the above article. They wrote that T cells, B cells, and natural killer (NK) cells interact with each other and with a diverse array of “accessory cells” such as monocyte-derived cells to generate an immune response. The NK cells are essential in the early phases of immune responses to viruses and malignancy.
Since vaccines derange these elements of the immune system, it is not difficult to understand why they are implicated as causal agents in all those modern ills of children, such as asthma and allergies, a number of cancers, gastrointestinal problems, autism and other behavioural problems to mention just a few so-called “new” diseases. In summary, there is a wealth of scientific data to demonstrate that vaccines cause serious derangements of all systems of the body, which result in serious injuries, including deaths, and in babies in particular.
The above is some of the strongest support for what many of us (especially RFK Jr) have been saying for years – that, beyond the infant deaths caused by vaccines, so can the shocking rise of innumerable chronic illnesses plaguing our society and children.
Confidential Report From Glaxo Smith Kline Revealed in Italian Court
Hang in and hold on, folks, because it gets even darker here (and will do so even more later in this post when we get to “hot-lot cover-ups”). In 2011, GlaxoSmithKline (GSK) produced a confidential report on SIDS, which was only made public following a decision by the Italian Court. Sudden deaths that occurred within 20 days after their hexavalent vaccination were tabulated (Hexavalent = DTP, Polio, Hib, HepB). The manufacturer concluded that the number of sudden deaths reported after receipt of its hexavalent vaccine did not exceed the background incidence or expected number of cases.
**Note that,although Miller cited this confidential report above in his bibliography, I can find no active public link to it currently (and the Wayback Machine has not indexed that page). In another paper, the report is also referenced on the following blog website, but I was unable to gain access.
Problem – this conclusion was not reflected in GSK’s own data! According to Miller, as shown in Table 36 on page 249 of the confidential report, the data indicate that 62.7% of these deaths occurred within 3 days post-vaccination, and 89.6% occurred within 7 days post-vaccination. Perhaps more significantly, 97 % (65 of the 67 reported infant deaths) occurred in the first 10 days post-vaccination, while just 3% (2 of the 67 infant deaths) occurred in the next 10 days. Additionally, 6 of the eight sudden deaths in children during their second year of life occurred in the first 3 days post-vaccination. Read it and weep:
Glaxo Smith Kline Does It Again
The above report was from 2011. GSK pulled the same crap in 2015, when they submitted another Periodic Safety Update Report (PSUR) to European vaccine regulators (I found it with difficulty). Table 6 on page 445 of that report shows that 52.5 % of these deaths clustered within 3 days post-vaccination, and 82.2 % occurred within 7 days post-vaccination, remarkably similar to the main findings in the Miller paper (and their previous report). Table 7 of the report shows that, again, 97.9% of all sudden deaths following the first dose of hexavalent vaccination (four doses are recommended) occurred within the first 10 days post-vaccination, while just 2.1% occurred in the next 10 days.
Despite these apparent warning signals, the vaccine manufacturer, GSK, concluded that its multi-dose vaccine was safe, and the European Medicines Agency (EMA), the regulatory authority responsible for overseeing vaccine safety in Europe, accepted the report at face value. No wonder Bobby fired the whole ACIP committee (because he is sick of this $%#!).
Two researchers (Puliyel and Sathyamala) later wrote a paper critical of Glaxo’s claims regarding vaccine safety (note that this paper can no longer be found at the Indian Journal of Medical Ethics (IJME) where it was initially published. The last time that paper can be found on the IJME website is on April 8th, 2025, using the Wayback machine here. They reported that:
Glaxo’s CEO tacitly admitted that there was no active surveillance during the post-vaccination period and only sudden deaths spontaneously reported were included under the heading of “observed” deaths. Thus, observed deaths following hexavalent vaccination were underestimated.
Glaxo compared observed deaths to a purported baseline of “expected” deaths. But expected deaths were based on the number of vaccine doses distributed. The report acknowledges that all doses of the vaccine distributed were not necessarily administered. Thus, expected deaths are likely to be inflated.
Glaxo’s baseline of expected deaths followed decades of widespread immunization campaigns, not a true baseline of SIDS cases in unvaccinated children or during the previous era when comprehensive vaccine programs did not yet exist.
Even worse is what they wrote in their introduction:
We analysed the data provided in the PSURs. The deaths acknowledged in the PSUR 16 were deleted from the PSUR 19. The number of observed deaths soon after vaccination among children older than one year was significantly higher than that expected by chance once the deleted deaths were restored and included in the analysis.
The CDC Pulls The Same Crap
In 2015, the CDC (Moro et al.) characterized the leading causes of death reported to VAERS from 1997 through 2013. The most common cause of death among 1244 children was SIDS. Most SIDS cases were among infants 2–4 months of age. Among the 1,165 infant reports, 86.2% received multiple vaccines prior to death. The median onset interval, the period from vaccination to death, was 2 days. SIDS reports were most common among children who had received DTaP, hepatitis B, inactivated polio, Hib, and pneumococcal vaccines simultaneously prior to death.
Despite these findings, CDC authors concluded that “no concerning pattern was noted among death reports submitted to VAERS…. The main causes of death were consistent with the most common causes of death in the U.S. population.”
I want to punch a wall right now.
The WHO Gets In On The Game
Here, unsurprisingly, the WHO also participates in the cover-up. Check this out, per the paper above (note Puliyel is again the lead author):
In 2018, the WHO revised the classification of adverse events following immunization (AEFI). Only reactions that had previously been acknowledged in the trials done for approval can be classified as vaccine–product–related reactions. Deaths observed during post-marketing surveillance are then not considered as ‘consistent with causal association with vaccine’.
Ed: Palm to forehead here, folks.The old “Catch-22”:
If any vaccine caused a significant increase in deaths in the trial done for approval, it would not have been licensed. Therefore, under this rule, any deaths that occur post-approval would, by their new definition, have to be classified as ‘coincidental deaths/events’ or ‘unclassifiable’, and no association with the vaccine would be acknowledged.
It just doesn’t end.
The Disinformation Response
As damning as the above papers and health agency actions are, please do not be surprised that there are several papers over the last 30 years (Hoffman 1987, Griffin 1998, Eriksen 2004, and Venneman 2007) that have concluded either; 1) there was no such association between vaccination and death or 2) that vaccination actually decreased the rates of SIDS. Yup.
The Worst Type of “Fake”
Recall the definition of the Disinformation tactic called “the Fake” above, the chief example of which is the designing of trials with “pre-determined results.” Those infuriate me beyond belief (see my chapter, “The Big Six,” in my book, “The War on Ivermectin,” where I detail the fraud and manipulations of the six largest trials on ivermectin in Covid). But there is another “Fix” tactic that triggers me even more – when “they” publish a study where the data presented in the paper contradicts the conclusion written in the abstract.
The worst, and absolutely worst, example of this tactic in the ivermectin war was the Oxford University trial, which I detailed at length in this post. In terms of covering up deaths associated with the vaccine, the below paper by Griffin et al stand out (note that it was published in the #1 ranked medical journal in the world, The New England Journal of Medicine) and is often cited (like a lot, especially by Gorski) as “proof” that no association exists between DPT vaccination and infant death exists:
From Schreibner et al (paraphrased for brevity)
Griffin et al concluded that their data do not show a causal link, but a proper tabulation of their raw data, looking at 4 groups of babies who died after DPT and Polio vaccination, shows the following:
Group 1 included babies aged 1.5-2.5 months (in the USA, they start vaccinating at 6-8 weeks). The majority of these babies died within 8-14 days, and they died after the first dose.
Group 2 included babies aged 2.5-4 months, who died after the second dose of DPT and OPV; the majority died between 15 and 30 days.
Group 3 included babies aged 4-8 months who died after the third dose. The majority died more than 31 days after vaccination.
Group 4 included babies who died aged 8- 12 months; these are the residue of delayed deaths after the third dose.
Far from showing no evidence of a causal link between the administration of DPT and OPV vaccines, the tabulated raw data by Griffin et al. (1988) reveal three important observed phenomena: 1. Younger babies die earlier than older, larger babies who take longer to die. 2. Sensitisation: increased immunological reaction (anaphylaxis) after subsequent doses of vaccines, 3. Increased numbers of deaths with the increasing interval from vaccination — delayed reactions, which are the rule rather than the exception.
I find the above a novel insight because it identifies a new pattern of death for infants vaccinated outside the 2-4 month window (when most die) – the older, “bigger” babies take longer to die in reproducible patterns. This instead allowed the authors to conclude “no association” exists. Brilliant.
COVID-19 Lockdowns Decreased Infant Mortality By Protecting Them From “Wellness Visits.”
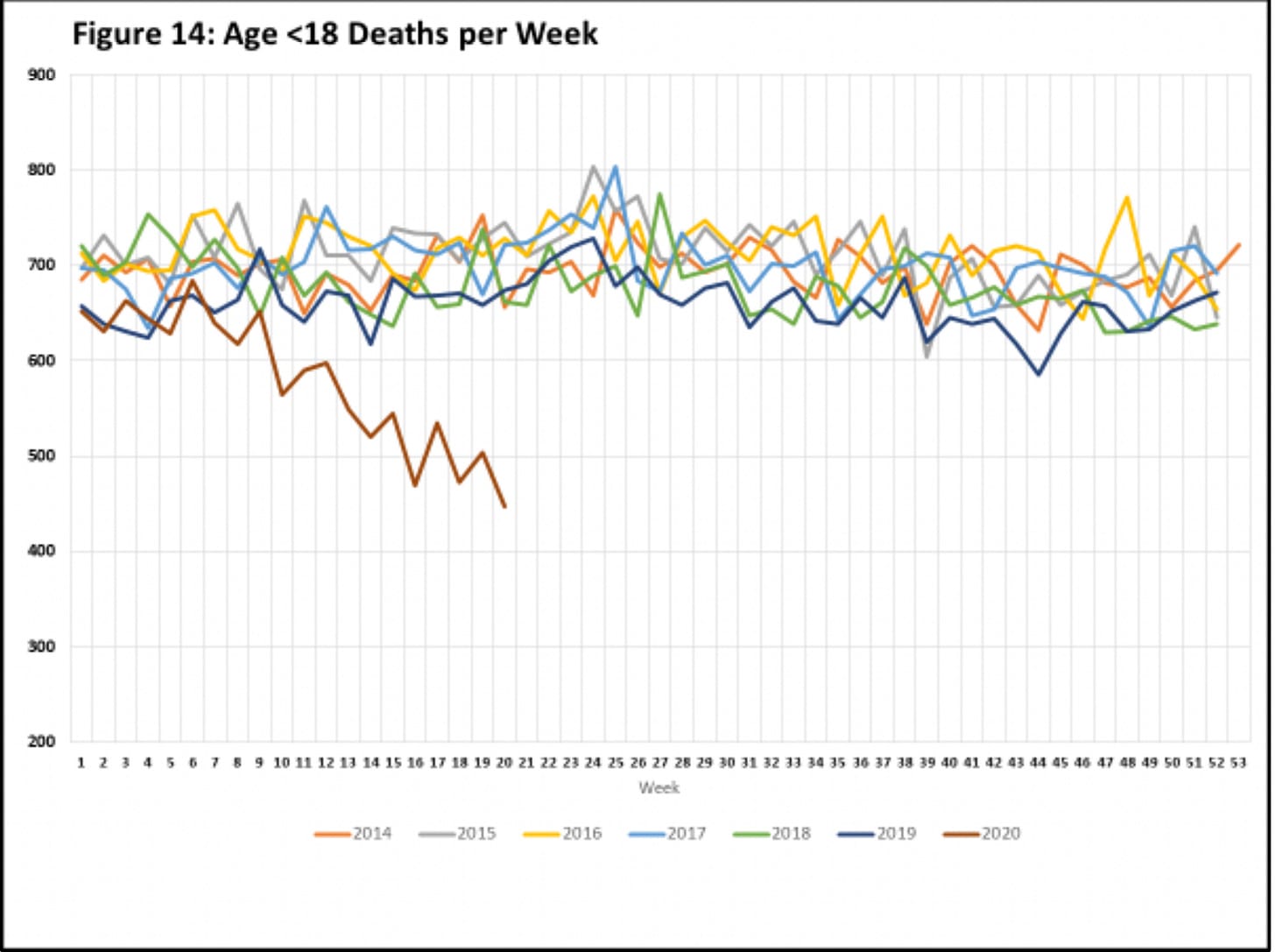
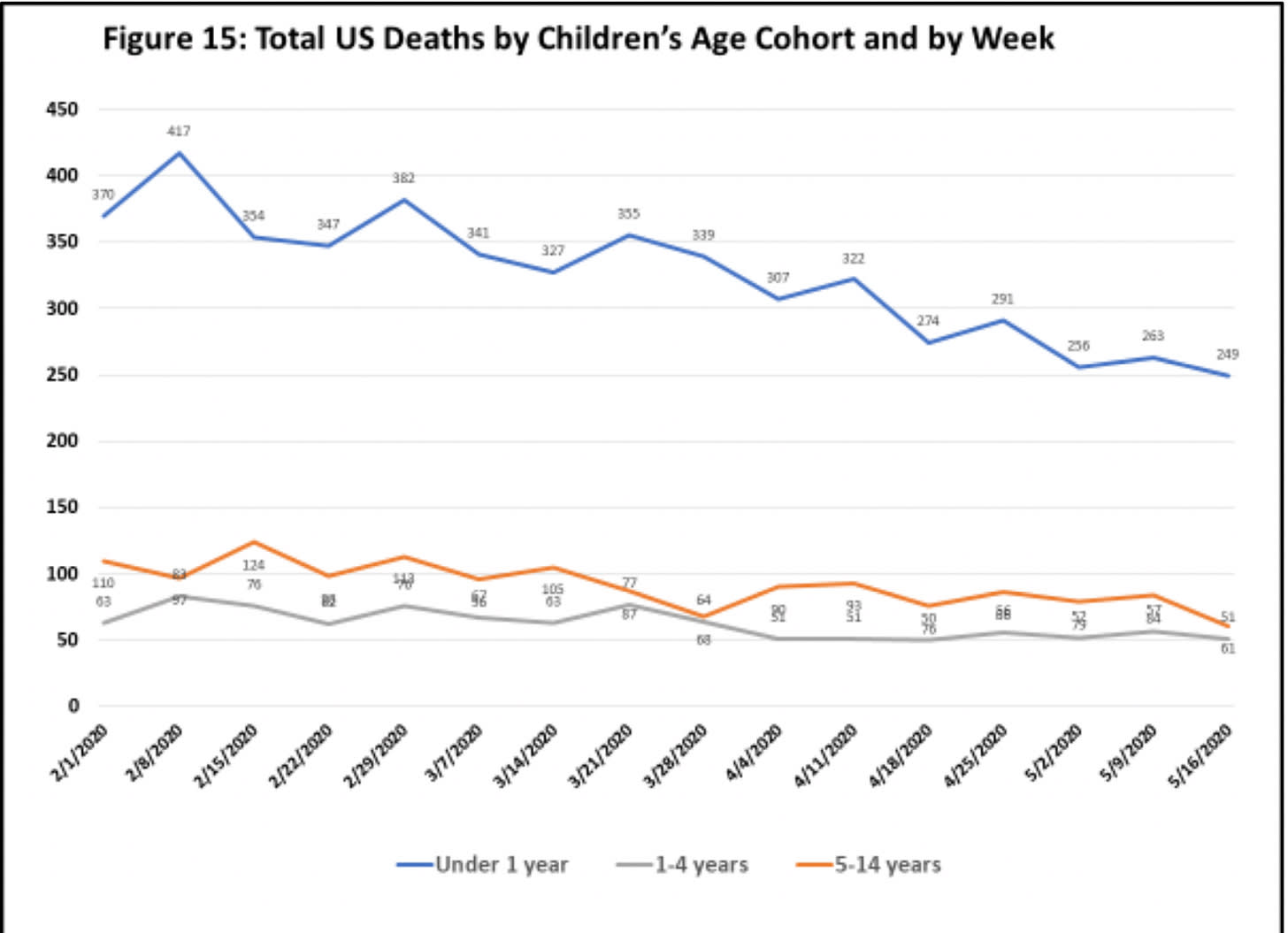
According to the Liberty Beacon article above, in 2020, something extraordinary happened—the lockdowns led to America’s first significant drop in vaccination rates, as well as a decline in well-child (vaccination) visits, which were deemed “non-essential.” AMD maintains that in their circle of vaccine experts, “many predicted this would lead to an unprecedented drop in SIDS rates.”
But only in children at the ages when SIDS typically occurs:
Furthermore, due to the political climate in Florida in 2021, the state’s childhood vaccination rate decreased from 93.4% in 2020 to 79.3% in 2021. At the same time, all-cause infant mortality under one year of age in Florida also reduced by 8.93% (a reversal of the 2020 trend, where infant mortality had increased by 0.67%). A 14 percent decrease in vaccination coverage was associated with a 9 percent decrease in infant mortality, suggesting roughly half of the infant deaths in Florida could potentially be attributed to vaccinations.
Do Vaccines Other Than DPT Cause Infant Deaths?
The short answer is yes (see Glaxo’s hexavalent subterfuge above – which includes DPT though), but also from the table below, taken from Miller, note the overall consistent temporal association between vaccination and death:
Can also read this disturbing legislative testimony from 1999 by Philip Incao, MD. He makes an absolutely compelling case linking SIDS to the hepatitis B vaccine.
A senior colleague of mine that I met during my Covid journey (one of the world’s experts on testosterone therapy and was a brilliant mentor to me in devising Covid vaccine injury protocols) is Dr. Eugene Shippen. Gene is a polymath Family Practice physician, expert in OB-GYN, Pediatrics, Medicine as well as Occupational Medicine and, in particular, Endocrinology. He became best known for his national and international lectures on male and female hormone replacement therapy. He is 83 years old and his practice now spans 55 years (he was also a trophy winning scratch golfer in his 40’s which pisses me off :).
You might be interested in my 4 cases of SIDS after reading your post. I delivered babies for the first 4 years of my Family Practice, about 400 mostly inner city welfare patients who used our hospital clinics – many had zero care before deliveries! I had 10-15% private patients, all of whom were following the rules. Out of the 400, I had two completely normal prenatal care experiences, deliveries, and healthy initial exams. Two died in the hospital nursery or the mother’s room 24 hours after receiving HepB immunizations. The staff reviewed everything and determined they were SIDS deaths, with no mention of vaccine reaction as a possible cause. W(hy)TF are we giving newborns with zero risk of the disease (Mothers all screened for HepB and negative)? In retrospect, they were vaccine deaths unreported. Two other cases were 2-3 months old after receiving DPTs at some close interval; again, no mention of vaccine reactions was made. One of the siblings of one case got a severe CNS reaction right after the jab and learning disabilities afterwards. I hope RFK Jr. can break the barrier with his team of scientists.
The conclusion of the Miller paper is about as strong a statement that you can find in the peer-reviewed literature:
While this paper does not prove an association between infant vaccines and sudden infant deaths, it reveals unusual patterns and safety signalshighly suggestive of a causal relationship.
Amazing that he got away with writing that.
“Hot Lots” And The Criminal Depravity Of The Pharmaceutical-Governmental Complex
Another factor contributing to the lethality of vaccinations is the manufacturing process. Many things can go wrong that could result in a lethal vaccine product. Unfortunately, hot lots are only diagnosed when “clusters” of deaths occur with the same lot number. “Hot lots” have been a feature of vaccines since their inception, a topic well covered by A Midwestern Doctor in their exhaustively documented post “The Century of Forgotten Vaccine Hot Lot Disasters.”
If interested in the dark history of vaccine hot lots and the many, many deaths and diseases they spawned (not only in the U.S but from several other countries), I suggest you read AMD’s article above. For this post, I want to focus on just one of them to illustrate the concerted, and I would argue, criminal actions taken by vaccine manufacturers and public health agencies to conceal deaths associated with vaccine hot lots.
For the sake of brevity and focus, I will leave out the topic of hot lots with the COVID mRNA vaccines, which I maintain underlie the majority of the millions of deaths from mRNA vaccines worldwide, as shown in studies from Belgium, New Zealand, the Czech Republic, and Japan. In fact, one could argue (most expertly done by Sasha Latypova) that the manufacturing process of the mRNA vaccine led to the near entirety of them being “hot” (i.e, lethal) to varying degrees. AMD does an excellent job of detailing the evidence of that disaster at the end of this post.
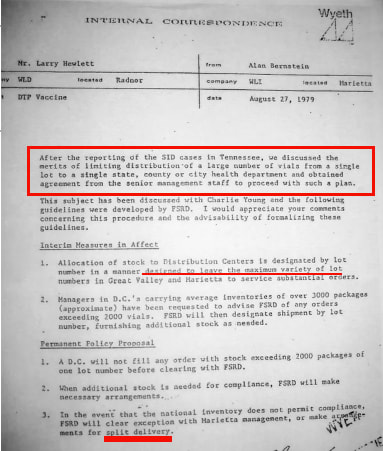
The Tennessee Hot Lot Disaster of 1978-79
The most damning event occurred in 1978-1979 in Tennessee. 11 babies died within 8 days following DPT vaccination. Five of the babies died suddenly within 24 h of vaccination. Nine of the 11 babies had received their vaccine from the same lot. A subsequent investigation confirmed a greater-than-expected relationship between Lot #64201 of the DPT vaccine and SIDS. Initially, health authorities “did not feel that a causal relationship could be totally excluded.”
FDA Response
However, later, the Food and Drug Administration (FDA) issued a revised statement that “experts (Ed: ugh) did not find evidence of a cause-effect relationship.”
CDC Response
The good ole’ CDC then claimed that the SIDS cases in Tennessee that occurred shortly after DPT vaccination were all a “coincidence.” A %^&#! coincidence, yes, you read that right.
Here is where the criminal depravity comes in (and continues to this day). From Miller:
After this incident, internal memos from the vaccine manufacturer revealed a new policy of limiting shipments of DPT vaccine, ensuring that no geographical location would receive all of the product from a single lot, thereby complicating the ability to trace hot lots that might cause clusters of SIDS cases post-vaccination.
The Wyeth (now Pfizer) memo, which spawned this diabolical response:
In essence, Wyeth decided that since it was impossible to avoid producing hot lots, the best solution would be to distribute the lots nationwide, making the deaths from it less apparent (which mirrors the common industry mantra: “the solution to pollution is dilution”).
There are no words.
A Glimmer Of Hope – And Further Evidence of Causation
In 1998, Ridgway reviewed vaccine injury compensation claims filed with the Vaccine Injury Compensation Program (VICP), which is notoriously difficult to obtain compensation through. However, of 107 claims that led to early death following DPT vaccination, 73 (68.2 %) were awarded compensation. In 50 of the 73 compensated claims, autopsies had attributed the deaths to SIDS. In contrast to the court of academia, in a court of law, 68% of claims of death resulted in compensation.
Here is one example of sanity prevailing from the vaccine court:
In 2017, the United States Court of Federal Claims issued a decision with regard to a claim filed with the National Vaccine Injury Compensation Program. An African-American male infant, J.B., received seven vaccines at his 4-month well-baby visit. On the following day, he died during his nap. The medical examiner stated that the cause of death was SIDS, and it was “natural.” Expert testimony by Dr. Douglas C. Miller, a neuropathologist, explained that when you receive one or more vaccines at once, as J.B. did, it evokes the production of cytokines. Physiological studies have shown that these can produce fever and inhibit the activity of 5-HT neurons in the medulla,causing prolonged apneas and interference with auto-resuscitation. Dr. Miller noted that J.B. was a “healthy infant…developing normally.” He was “immunologically normal.”
Special Master Thomas L. Gowen issued his decision: “I have concluded that the petitioners have demonstrated by a preponderance of the evidence that the vaccines can and likely did play a critical role in this child’s death by stimulating the production of inflammatory cytokines that suppressed the respiratory response system and caused the vulnerable infant to be unable to respond in the normal way to the accumulation of carbon dioxide in his system. The role of inflammatory cytokines as neuromodulators in the infant medulla has been well described. It is likely the reason for a significant number of SIDS deaths occurring in conjunction with mild infection. I have concluded that it is more likely than not that the vaccine-stimulated cytokines had the same effect in this vulnerable infant during sleep. Accordingly, petitioners are entitled to compensation. A separate damages order will issue.”
Conclusion
I maintain that the global suppression of vaccine-induced infant deaths by public health agencies is not just a matter of bureaucratic oversight or scientific debate—it is a calculated campaign of obfuscation, misdirection, and denial that has persisted for decades. Recall the notion that, from the Watergate scandal, “the cover-up is the crime,” which encapsulates the idea that efforts to conceal wrongdoing can be as incriminating as, or even constitute, the primary offense itself.
Through strategic reclassification of causes of death, removal of vaccine-related mortality codes from international diagnostic manuals, and relentless messaging to dismiss any link between vaccines and sudden infant deaths, these agencies have prioritized the preservation of vaccination programs over the lives and voices of the most vulnerable: our infants and their families.
The stark rise of SIDS and SUID diagnoses following the expansion of immunization programs, the shifting of blame to improbable causes like “suffocation in bed,” and the systematic erasure of dissenting data from both the scientific record and public discourse expose a machinery more invested in protecting its own interests than in safeguarding public health. Until these patterns of deception are confronted and rectified, the tragic toll will continue, hidden not by lack of evidence, but by the willful suppression of truth at the highest levels of public health authority.
I leave you with this quote, from Dr. James R. Shannon, former Director of the National Institutes of Health who declared, “the only safe vaccine is one that is never used.”
If you find value in the time, research, and care I invest in crafting these posts to expose critically important truths about the safety and efficacy of a diverse set of medical therapeutics, please support my work with a paid subscription.
Looking forward to speaking at David Martin’s REJUVEN8 Health Summit on August 1-2, 2025. Come one, come all if you can. Register by clicking the image below, website with agenda and speakers is here.
This content is courtesy of, and owned and copyrighted by, https://pierrekory.substack.com and its author. This content is made available by use of the public RSS feed offered by the host site and is used for educational purposes only. If you are the author or represent the host site and would like this content removed now and in the future, please contact USSANews.com using the email address in the Contact page found in the website menu.