Story at a Glance:
•One premier research group has bravely studied the vaccine-injured and provided many critical details about their multi-year illnesses.
•Unfortunately, despite their excellent research, medical journals have refused to publish their results, including the most recent study which showed clear differences exist between long COVID and COVID-19 vaccine injuries.
•Science is ultimately predicated upon the methods we use discern what is actually true (epistemology). As this subject has been neglected, our epistemological standards frequently result in existing dogmas and vested interests being reaffirmed while critically important data never reaches the public awareness (e.g., due to widespread medical journal censorship).
•During COVID-19, the severe abuses of the scientific community (which ultimately resulted from it having no accountability for failing to uphold its social responsibilities) broke the public trust in science, and allowed something previously inconceivable—MAHA to gain control of our corrupt scientific apparatus and have a mandate to reform it.
•NIH director Jay Bhattacharya has announced his commitment to fixing the scientific apparatus and has engaged in a variety of NIH initiatives and public discussions which are vital to allowing science to serve the people rather than vested-interests.
Yale’s medical school is widely considered to have one of the top autoimmunity research and treatment programs in America. As long COVID is considered to be immunological in nature, their researchers extensively studied it, and remarkably some of them then pivoted to also studying vaccine injuries (in part because the COVID vaccines rather than curing long COVID patients, sometimes made them much worse). A few days ago, they finished a new research paper on the subject, but like their previous ones, it was immediately summarily rejected by the “reputable” journals it was submitted to (including the one I feel was the most obligated to publish these findings). In this article, I aim to cover the importance of their most recent results and, more important, examine what their habitual censorship reveals about science in general.
Yale’s LISTEN Study
All of this research was conducted within Yale’s LISTEN Study (Listen to Immune, Symptom and Treatment Experiences Now) where a group of patients with both long COVID and then COVID vaccine injuries were extensively followed, evaluated (e.g., for symptoms and biomarkers) then analyzed to develop a consistent clinical picture of the diseases. As this is an extremely important study. I’ve been in touch with participants throughout the study, who’ve shared data consistent with our observations of vaccine-injured patients over the last four years.
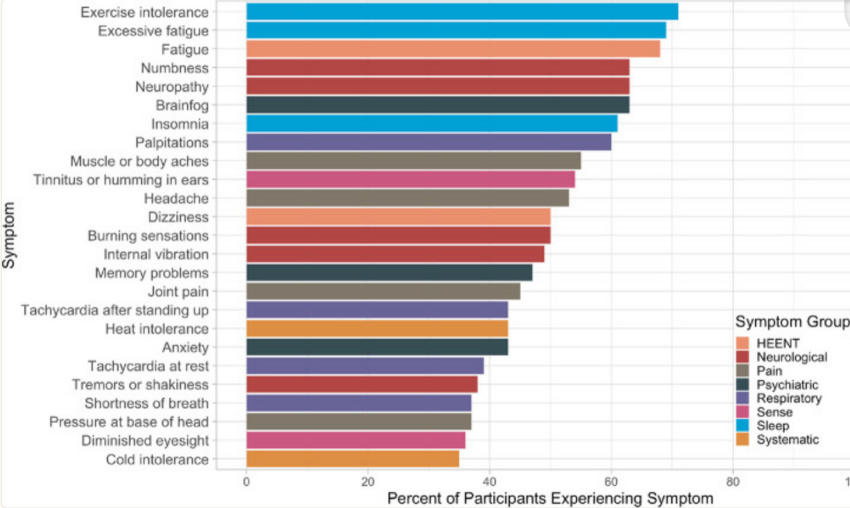
Initially, in 2023, they shared some of their preliminary data as a November 2023 preprint (which has still not been accepted for publication) which detailed the common symptoms seen in the 241 participants with post vaccination syndrome (PVS), which match what we’ve seen in clinical practice:

To quote the study:
In conclusion, people reporting PVS after covid-19 vaccination in this study are highly symptomatic, have poor health status, and have tried many treatment strategies without success. As PVS is associated with considerable suffering, there is an urgent need to understand its mechanism to provide prevention, diagnosis, and treatment strategies.
Note: these results were discussed in more detail in this October 2023 online conference (e.g., the mast cell component of the illness). From watching this conference, my impression was that the investigators sincerely want to help the trial participants, but due to the unpleasant implications of their findings, are in a very challenging position (hence why their 2023 pre-print has still not been published).
In February 2025, they published a much more detailed study, that unfortunately also remains a preprint (as no journal would publish it). It was comprised of 42 post-vaccine syndrome (vaccine-injured) participants (and 22 controls) and detected a variety of concerning changes. These included lower CD4 cells and elevated TNFα+ and CD8 T cells (which equates to a picture of immune suppression and autoimmunity). Additionally, post-vaccine syndrome (PVS) participants had a tendency for the re-activation of chronic infections and had a chronic persistence of the spike protein. The more detailed data was as follows:
General Health
Vaccine-injured individuals reported lower general health scores, such as lower physical function scores, higher anxiety, depression, fatigue, and pain scores and increased sleep disturbances.
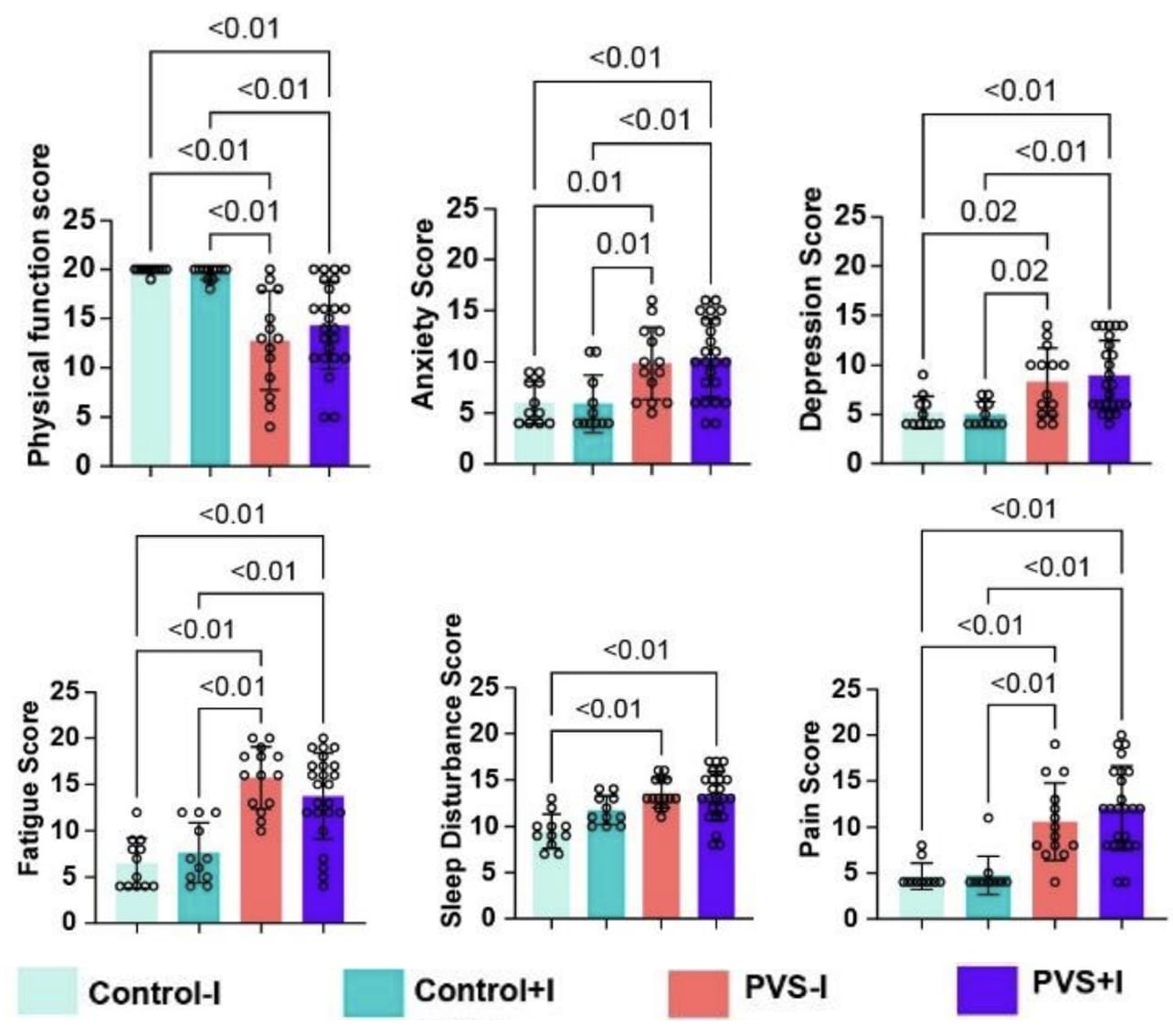
This is important because it demonstrates that vaccine injuries are a real condition with actual health effects (rather than just ‘being in your head’).
Spike Protein Persistence
To my knowledge, their second study provides the best demonstration that the COVID vaccine persists for a prolonged period within the body and when present, typically is much higher than in controls.
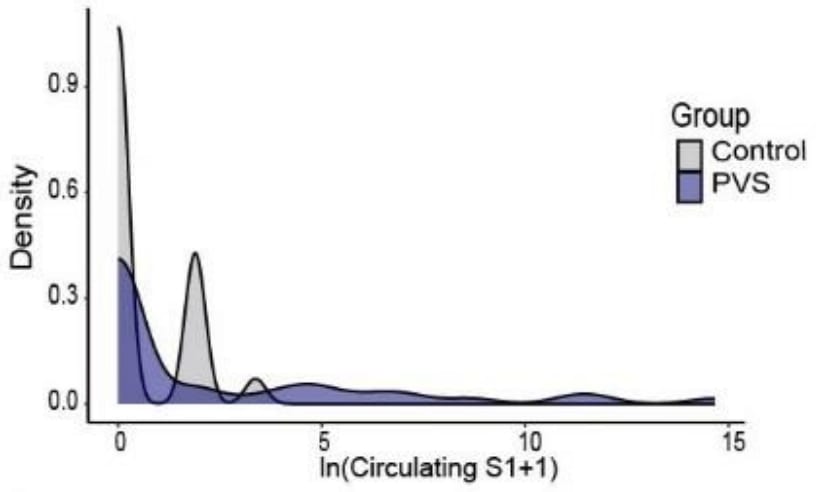

This data collectively shows that:
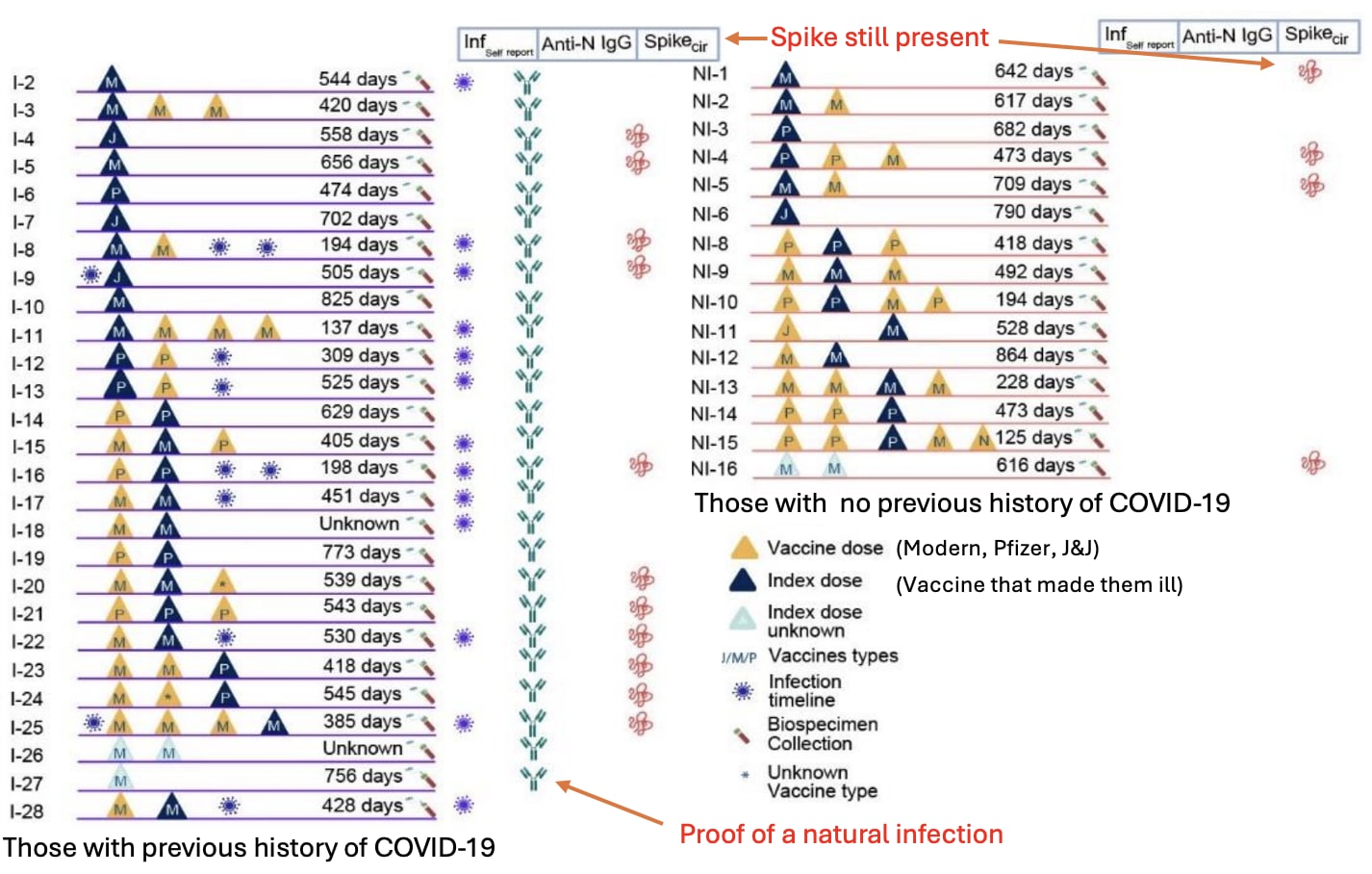
•The COVID vaccine spike protein can persist for years in the body. The major limitation with each previous study was that spike was still found at the end of the study duration, so it was not possible to know how long it actually persisted. As this study shows, a few months was not long enough to measure the spike protein’s persistence, as in some cases, it lasted for close to two years (and were it to be measured again, might last even longer).
•In many cases, COVID spike protein persistence eventually stopped but symptoms continued. Assuming this is correct, that means in many cases the vaccine will eventually be eliminated (which may depend upon the vaccine lot they received), and that not all of the post-vaccine symptoms are a result of persistent spike protein production.
•The persistence of the spike protein without any proof of a natural infection provides strong evidence the vaccine’s spike protein is what’s persisting in the body.
Note: numerous other studies (discussed here), the earliest of which was a March 2022 one by Stanford, have also shown the COVID vaccine persists in the body. While this persistence is typically attributed to the vaccine mRNA integrating with the host’s DNA (which does happen), leading to perpetual mRNA production, both I and Dr. Malone (a leading expert in this area) believe the primary (and far more probable) source of persistence was the mRNA being modified to resist degradation (leading to the vaccine mRNA indefinitely producing synthetic spike protein in the body).
This, in turn, was a result of needing to ensure the vaccine persisted long enough to produce sufficient spike protein to produce a vaccine immune response (and hence win an approval) but this being incredibly challenging to do (especially given the rushed nature of Operation Warp Speed and how many companies were racing to get the initial approval and the billions in profit that would follow). Consequently, developers prioritized maximizing the mRNA vaccine’s persistence and productivity, given its unpredictable behavior in the body and to accept that the injuries which followed from excessive spike production within the body were an acceptable price to pay for expediting the vaccine (hence illustrating why blanket liability shields, such as the ones given during Operation Warp Speed, are so problematic).
Immunologic Suppression and Viral Reactivation
One of the major problems with the COVID vaccine has been that it causes a significant number of people to develop signs of immune suppression, such as frequent flu infections or reactivation of chronic viral infections (e.g., shingles in general along with severe cases of shingles has been strongly linked to vaccination).
Note: less severe versions of this immune suppression have also been observed to follow shedding exposures.
A variety of theories have been put forward to explain why this happens, such as:
•The immune system being locked onto the vaccine antigen, which results in it losing the ability to target other natural antigens (and has been proven to be an issue with many other vaccines as well).
•The vaccine creating an IgG4 class switch, which essentially causes the immune system to no longer fight back against COVID spike proteins.
•The overstimulation of the vaccine over time causes a suppression of spike protein antibodies (which the study observed). This could either be a result of the vaccine-injured patients have an existing inability to develop immunity to the vaccine’s spike protein (as suggested by the January 2023 study) or that the vaccine gradually eliminated the body’s ability to bind to the spike protein, resulting in individuals becoming more vulnerable to the spike protein over time if they happened to have a long-acting vaccine continue to produce spike protein inside them.
•The spike protein collapsing the body’s zeta potential (which as it gets more severe can cause blood clots of increasing sizes). Since many symptoms of infectious illnesses result from the zeta potential collapse they create, those symptoms of illness are magnified when there is already an impaired zeta potential (which the spike protein has been shown to collapse).
•The spike protein directly destroying immune cells (e.g., CD4 cells—something also seen in HIV) and the stem cells that create the immune cells.
Note: these labs were sent to me by one vaccine-injured participant in the study.
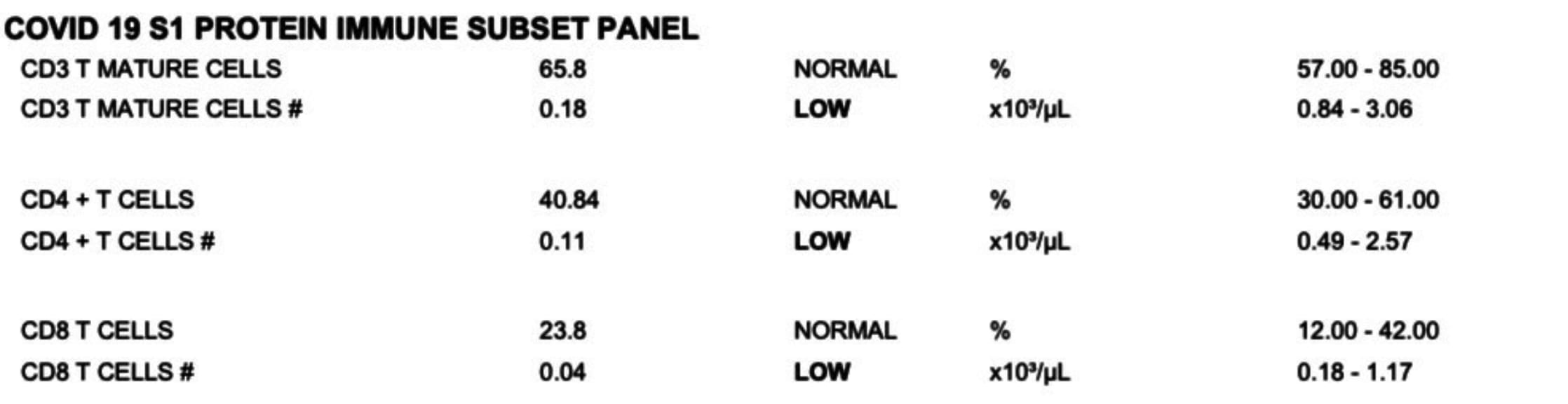
In addition to showing a loss of key immune cells, the study also showed both the CD4 and CD8 cells had signs of being “exhausted,” as changes were observed in them that are known to correlate with those cells partially losing ability to respond to infections due to a chronic over-activation of them (e.g., by persistent vaccine spike protein).
Finally, much in the same way that there were signs of immune dysfunction, the study also observed consistent significant signs of viral reactivations in the cohort, most notably with Epstein Barr virus, but also with herpes and frequently both concurrently (however for some reason, shingles was not assessed in this study). In turn, we have frequently seen EBV be a component of the vaccine-injury picture (to the point sometimes it needs to be treated) and frequently also observe an increase in herpes.
Note: one of the best treatments I have found for all three of these viruses is ultraviolet blood irradiation (discussed here). Additionally, DMSO can be quite helpful for shingles and herpes (discussed here).
Additionally, there was also a possible increase in seropositivity to a few other pathogens (e.g., H. Pylori and the parasite Toxocara), which could potentially (but more likely than not doesn’t) explain some of the gastrointestinal issues seen in vaccine-injured patients or their response to ivermectin.
Autoimmunity
One of the most common issues associated with the COVID vaccines were autoimmune disorders (detailed here) due to the fact the spike protein had an unusually high overlap with human tissue and because it was designed to express itself on the surface of human cells. In this study, Yale’s team reported:
We observed significant increases in IgM reactivities against 65 antigens, IgG reactivity against 1 antigen and IgA reactivities against 39 antigens in PVS compared to controls after multiple testing corrections. Among these antigens, two showed log₂fold change of greater than 2: anti-nucleosome IgM [which is strongly associated with lupus] and anti-AQP4 IgA [which is associated with a rare autoimmune disorder that attacks the central nervous system, particularly optic nerve and spinal cord].
Note: a significant increase in TNF⍺ levels in simulated CD8+ cells (which can often lead to immune dysfunction) and a non-significant increase in CD8+ IFNγ were observed.
I feel these results are important as they validate something many of us have been claiming for four years with the vaccines.
Note: less severe versions of autoimmunity have also been observed to follow shedding exposures.
Long COVID vs. Vaccine Injuries
As both long COVID and vaccine injuries result from spike protein exposure, they hence also have many overlapping symptoms. Because of this, the medical community’s approach to saving face with vaccine injuries has been to claim anything people attribute to a vaccine injury was actually “long COVID” (or simply COVID-19) and many in turn have accepted going along with this farce as it’s the only way “long COVID” vaccine-injured patients can get any type of support.
Note: long COVID was used to market the vaccine (either by claiming it could prevent you from getting long COVID if you later caught COVID-19 or treat it by increasing your immune response to a persistent COVID infection, thereby eliminating it). Unfortunately, the opposite happened (e.g., we know many long COVID patients who became much worse after being given a vaccine), and conversely, we also saw many vaccine-injured patients become worse after subsequently getting COVID (or even just being exposed to someone who’d been vaccinated and was shedding the infection).
In their most recent August 2025 publication, Yale’s team took all their data and used an AI analysis of it to compare the outcomes and symptoms of long COVID patients (on average at day 447 of their illness) to Post-vaccine Syndrome cases (on average at day 595 of their illness). From this, they found:
•Among the people with long COVID, 54% described their health as fair or poor; and among those with PVS, 44% described their health as fair or poor and with symptom severity on worst days being similar between groups.
Note: our experience has been that in most cases, the symptom severity for vaccine injuries is much more severe than long COVID (and likewise harder to treat).

•Participants with long COVID most commonly reported brain fog, altered sense of smell and taste, shortness of breath, fatigue, memory problems, and difficulty speaking (many of which are classic signs of a COVID infection).
•Participants with PVS (post vaccine syndrome) more frequently reported burning sensations, neuropathy, and numbness (all of which are very common in PVS), and since the pandemic began, significantly more new diagnoses of neurologic conditions.
Note: a much more detailed list was published of new diagnoses which occurred in the study group, where in addition to neurologic conditions (including seizures, dementia, multiple sclerosis, Parkinson’s, neuropathy, small fiber neuropathy, etc.) which increased 2.07X compared to long COVID, increases were also seen in liver disease (3X), cardiovascular diseases including strokes (2.5X), Lyme disease (2X), Mast Cell Disorders (1.71X), EDS (1.5X), becoming immunocompromised (1.285X), and various autoimmune disorders (1.25X). However, except for a high number of Mast Cell Disorders and Neurologic diagnoses, these proportional increases occurred in a relatively small number of people.
•The most important discriminative symptoms for the two syndromes were altered sense of smell, cough, burning sensation, and brain fog.
Note: 85% of long COVID patients and 63% of PVS patients reported brain fog. In our experience, we find brain fog to be one of the most common PVS symptoms.
•Clustering analysis identified three distinct symptom clusters. Cluster A (7.4% of all participants, 72% PVS) primarily included neurological symptoms. Cluster B (58.0% of all participants, 65.7% long COVID) exhibited widespread symptoms across the categories of Pain; Head, Eyes, Ears, Nose, and Throat; Respiratory; Gastrointestinal; Systemic; Dermatologic; and Sense. Cluster C (34.6% of all participants, 71.5% long COVID) featured predominantly psychiatric and sleep-related symptoms. Cluster stability was confirmed through repeated subsampling, demonstrating an average overlap of 90.7% to 97.6% across clusters.
The study then concluded:
Three distinct symptom-based subgroups, including one enriched for PVS and dominated by neurological symptoms…supports the hypothesis that while both conditions may involve immune responses to the SARS-CoV-2 spike protein, additional mechanisms—such as direct viral tissue effects—may be more relevant in long COVID. For example, disturbances in smell and taste may reflect local infection of olfactory and gustatory tissues. The ability to distinguish these syndromes based on symptomatology reinforces the notion that they may arise, at least in part, through different biological pathways
These diagnostic ambiguities highlight the need for validated biomarkers and greater clinical awareness of both conditions. Also, future research should prioritize longitudinal studies and immune phenotyping to validate findings, clarify mechanisms, and improve management strategies. The clear symptom differentiation identified provides an important step towards personalized treatment for individuals with long COVID and PVS.
In conclusion, long COVID and PVS appear to be distinct syndromes with partially overlapping but differentiable symptom profiles.
Epistemology
Epistemology is a branch of philosophy which seeks to determine how we ascertain knowing if something is true. In turn, I would argue there are essentially three different standards an epistemological system can be held to:
-
It fulfills a role that allows society to function smoothly.
-
It has some type of corrective mechanism that allows it move closer to the truth and further away from falsehoods.
-
It has a way to unravel the actual truth of our reality.
Of these, the first receives the greatest priority, and hence most consistently shows up throughout history, the second is the mark of “better” epistemological systems (and typically births successful societies), while the third is where my own interest resides (and is often where profoundly impactful discoveries originate from).
Note: these three concepts also extend to things beyond science. For example, society largely cannot function without money as an agreed upon unit of exchange is necessary to motivate, facilitate, and streamline many of the essential processes the society relies upon. Yet, without a strong corrective mechanism, government money often loses its connection from reality, leading to massive overspending, overprinting (to cover that overspending), and then inflation proportional to that overprinting (making more and more of the population no longer be able to afford their needed expenses). Finally, if you take a step back, a good case can be made that money rewires our hearts and minds to view “making money” as the reason for existing, when in reality many far more important things exist to nourish our souls (and likewise forget other viable options like homesteading, a barter economy or that tightly-knit supportive communities like the Amish exist which can allow one to partially “opt-out” of the monetary system).
One of the major problems most epistemological systems run into is that being an arbiter of the truth has a lot of power attached to it (hence why the first standard I listed appears throughout history). Likewise, one of the most common battles which occurs is attempting to transition to the second standard (as those holding a monopoly on truth never want to relinquish their power), but typically eventually is successful, as once people have a monopoly on power (e.g., the truth) and no longer have outside accountability, they increasingly misuse it, eventually resulting in glaring problems existing within their epistemological system system outside revolutionaries can highlight to justify switching to the second standard (having a self-corrective mechanism for determining truth).
Unfortunately, since people always want power, the exchange between these two standards is far more mutable than people realize. For example, the scientific revolution was intended to be a revolution against the dogmatic restrictions of the society which prevented necessary truths (e.g., the earth orbiting the sun rather than the earth being the center of the universe) from being discovered. Yet, in just a few generations (particularly after World War II), after science rose to power, it became just like the dogmatic institutions it had replaced (leading to many arguing our modern form of science, “scientism” has become a religion seeking to monopolize truth no different from the restrictive faiths that proceeded it).
Determining Truth
Different branches of epistemology deal with different types of knowledge (e.g., how can you know something you believe happened actually happened). The branch I am the most concerned with (understanding the scientific principles which underlie our reality) essentially concluded:
•There are three ways you can discern truth: logically, through empiricism or by personal experiences (which are often mystical in nature).
•Logic is not reliable as a way to determine truth as it is often extremely subjective and prone to misinterpretation (e.g., one can rationalize almost anything and frequently get others to go along with it). Likewise, personal perceptions are not reliable either, as they cannot be replicated by others and may be prone to hallucinations or misperceptions.
•As such, empiricism (using repeated results to prove or disprove the constructs of reality) wins by default and should be the predominant epistemological standard, with “correctly structured” logic serving a secondary role to enhance the utility of empiric data (e.g., by providing a sensible way to interpret it).
Because of this, there has been a greater and greater push for data that has become increasingly dogmatic (e.g., no study counts unless it is a costly randomized double-blind trial) and many have observed science has increasingly lost its ability to accurately determine truth despite now having access to an insane amount of data.
Note: I personally believe logic can be extremely useful if it is more objective (e.g., not constantly morphing its baseline standards to ones that support a desired narrative) and “open-minded” (e.g., focused on trying to identify what’s true from the vast range of possibilities around us rather than trying to restrict reality to a narrow rigidly defined set of premises which affirm a desired outcome). Likewise, while I support empiricism, I feel its primary utility is for disproving theories rather than identifying what is true (so I frequently use empiric frameworks and datasets as a way to double-check I am not deluding myself). Finally, I believe a vast amount of critical knowledge can only be obtained through individual perception (provided its done in a sensible manner) and find it quite frustrating our society continually demeans this form of knowing (e.g., to gaslight those who know they were injured by a pharmaceutical), particularly since this means of discerning truth was responsible for some of the greatest scientific discoveries in history.
Epistemological Algorithms
In teaching, there are essentially two ways you can approach the task:
1. Rigidly structure everything so that exactly what the educational system feels need to be learned is learned in sequence and then students are repeatedly drilled on performing and executing what is expected at each stage—including not only the knowledge itself but also the cognitive algorithms they should use to apply it.
2. Inspire people to want to learn and give them both the tools and freedom to develop their knowledge as much as possible while lightly guiding them towards the critical points that need to be learned.
While I greatly prefer the second model, the first option is far more preferable and common, which I believe is due to a combination of the following:
•It helps establish the rigid hierarchy many running our society benefit from.
•It produces a more consistent (and hence replicable) final product—which is often needed for societal institutions to function).
•It’s much easier to do.
•It appeals to the innate human need to control things (e.g., schools give bad education outcomes in the graduates, so the “solution” is to force an increasingly tight grip upon the students to ensure they comply and assume a desired state rather than to re-evaluate the existing educational framework).
Conversely however, it stifles the ability of students to express their higher capacities and creativity and is woefully inefficient (e.g., as people often don’t learn very well in this model, they tend to be “taught” the same material over and over).
Note: when I was in middle school, I made an independent effort to learn, understand, and appreciate the concepts I learned (leading to long-term retention), and then was quite surprised at how much of what was taught in high school (and to a lesser extent college) was essentially the same material being retaught (and likewise during my medical education, the same things were repeated retaught). Since I did not want my brain to atrophy by repeating those lessons ad-infinitum, I spent more and more of my time learning other subjects I felt were useful to understand (including the Forgotten Sides of Medicine) and trying to effectively learn the material I was taught the first time it was shown so I had more time to study the other subjects I wanted to learn about (much of which was made possible by accidentally discovering how to rapidly memorize information in 7th grade).
In my eyes, the greatest problem with our accepted framework is that it (conveniently) destroys critical thinking and replaces it with algorithms (which intelligent individuals are often excellent at rapidly and flawlessly performing) that cannot be discarded when they are no longer useful. I will now highlight a few examples:
1. Over the years, many of my awake colleagues (e.g., those who do not follow the crowd off a bridge or can cure “incurable” illnesses) have noticed that in both competitive strategy games and in medicine, as participants get better, they get better and better at what you are supported to do (e.g., perfectly applying clinical algorithms), but simultaneously, they are quite bad at anticipating major problems a few steps down the road which are outside their algorithms (e.g., the best placers throwing a match because their “correct” move in the moment sets them up to be in an un-winnable situation five turns later).
In turn, since so many different possibilities exist of what can emerge in the future, it’s essentially impossible to account for all of them. Yet rather than try to foster a creative form of thinking and “open-minded” logic that facilitates this (and allows the subconscious to be aware of the possibilities and bring the conscious mind’s awareness to the critically important possible futures), this skill (“future echolocation”) is largely absent from our educational system.
For example, in medicine, some algorithms are very useful (e.g., rigid and well-designed algorithms prevent a lot of critically ill patients from dying). However, with many other ones (e.g., for chronic illnesses) you can frequently tell that if a patient is put onto that algorithm, they will just gradually get worse and need more and medical services (e.g., drugs or surgery) which cost a lot and create more illness. Because of this, if any focus is directed to future echolocation, it’s fairly straightforward to see the likely medical futures ahead of a patient early in their illness. However in many cases (particularly when a medical dogma is challenged), doctors can’t see that, and a key reason I adopted my current practice of medicine was that did not want to be forced to put patients onto algorithms I felt would lead to bad outcomes (but most of my colleagues supported).
Note: the primary reason I gravitated towards this style of thinking (e.g., future echolocation and embracing an ambiguous and uncertain future) is because I find it makes life much richer and more interesting.
2. Since there is so much benefit from controlling a society’s truths, a lot of work has gone into both crafting the algorithms individuals use to discern truth and monopolizing the datapoints used to fuel those algorithms.
For example, we are taught that the “most prestigious” form of evidence is the most credible, and as you might expect, a lot of work has gone into establishing certain “trustable sources” (e.g., premier medical journals) as the most credible ones, while simultaneously corrupting them so they will only promote messages that support preferred narratives (e.g., that the COVID vaccines are 1000% safe and effective).
Note: it thus is quite extraordinary the Yale publications are being repeatedly blockaded by the medical journals, as our system has has been structured for the premier journals to always march in lockstep with the premier institutions.
Much of this is highlighted by the “PubMed fallacy” I frequently observe when I try to expose a more orthodox colleague to an unconventional idea. In those instances, they will frequently respond by pulling up PubMed (the “best” source of medical information online), searching for the idea, and then after not seeing corroborating results on the first 1-2 pages, tell me “well there’s no evidence of _____ so I think that’s misinformation.” I however consider this a fallacy as:
•The journals indexed by PubMed tend to be those which affirm the narrative, so even if a journal is willing to publish a controversial paper, it frequently will be in one not indexed by PubMed and hence “not exist” (e.g., studies were conducted showing mRNA vaccine shedding occurred, but no PubMed indexed journal would publish them, and after years of work, the authors finally gave up and published them in a non-indexed journal—hence making the study “not exist” to much of the scientific community).
•Rather than think critically about a subject (much in the same way navigating ambiguous futures requires much more cognitive effort), individuals will frequently default to simplified algorithms where everything is done for them e.g., telling them how to play a game or how to treat a patient), despite that approach frequently leading to a bad outcome. The PubMed fallacy illustrates another aspect of this, as there, a (limited) algorithm takes over which spares the individuals from having to expend effort thinking about the subject by allowing them to believe they effectively solved the issue by quickly checking what headlines of PubMed indexed articles stated on the subject.
Note: in many cases the actual data in a paper will different from the brief PubMed summary of the article doctors typically read.
Now that AI is entering the fray, we are now seeing a further evolution of this mental laziness, where rather than trying to do a cursory review of the data on a subject, individuals will typically just ask AI to give them the answer, at which point (if the AI prompt is not worded correct), they will typically receive a regurgitation of the most referenced (i.e., narrative supporting) scientific perspectives on the issue, alongside a validation of their pre-existing viewpoints—in essence making AI frequently fail to provide the corrective epistemological mechanisms needed to bring us closer to the truth and further from falsehoods.
Note: AI can be extremely useful for researching topics if you ask it to tell you why you may be wrong or help reconcile contradictions you can’t understand (and explain why), but in most cases people instead ask to be validated (which AI systems default to so they can increase view time) or ask AI to figure everything out for them. Likewise, on topics that are now largely acknowledged by medicine (e.g., the dangers of benzodiazepines) they are very effective for getting the data you need, whereas in non-acknowledged areas, they are not (e.g., the DMSO series has taken so much time because virtually all of the studies I’ve used will not show up in AI queries).
All of this in turn is extremely challenging to navigate, but since I had already developed a sense of which areas of the internet would have which types of information I needed (e.g., Wikipedia and Reddit are useful for some but fairly useless for anything “controversial”) and when to be skeptical of what was presented online, it was fairly straightforward to transmit that skillset to the AI systems. However, as many (especially the younger generations) have not gone through that transition, I am worried this critical means for appraising AI data will be lost, and instead it will just greatly accelerate the trend towards mental laziness and a widespread loss of critical thinking.
Restoring Trust in Science
Prior to the pandemic, we watched a continual and progressive multi-decade decline in the global quality of science as every institution became increasingly hostile to anything being published which challenged mainstream narratives (e.g., the problems with vaccines or statins) and simultaneously became laxer and laxer in uncritically publishing industry studies (effectively make them nothing more than marketing material).
As such, like many, I gradually learned all the different ways studies are routinely doctored to provide a misleading conclusion that supports the narrative. Because of this, I eventually concluded that if a peer-reviewed supports the mainstream narrative, its results must be treated with skepticism, whereas, in the rare instances where something which challenges the narrative is accepted for publication in a major journal, it is highly likely its very accurate as it had to withstand a significant amount of scrutiny to make it to publication.
Note: at the first APIC meeting with new (less industry friendly) appointees, the panel voted 5-2 in favor of another mono-clonal antibody RSV “vaccine” as the existing data showed its benefits outweighed its risks (upsetting many in MAHA). Recently, Dr. Malone disclosed that the information on the vaccine was given to them by the CDC immediately before the meeting, and was structured to hide a significant seizure risk from the vaccine along with a significantly increased death rate in individuals who took it (all of which are techniques drug companies routinely do in papers they publish).
All of this kicked into overdrive during COVID-19, and again and again, we saw ridiculous and harmful policies (not supported by the existing evidence) be rammed down our throats by the public health bureaucrats, that when challenged, resulted in the skeptic being cancelled rather than any serious evaluation of the policy. Because of this, particularly with the COVID vaccines (due to both them being mandated and how transparent it became that they were neither “safe” nor “effective), a massive loss of trust in the scientific and medical apparatus followed.
While tragic, in many ways I am glad this happened, as for decades I’ve watched this situation worsen, but it did so at a slow enough pace that people did not revolt against it (instead tolerating the ever increasing number of medical injuries). As such, I felt the only thing that could potentially avert this slow-motion train wreck was a shift happening that was extreme it destroyed people’s trust in the medical system and the unquestioned faith science had coasted on for decades—which due to the medical industry’s excessive greed essentially happened during the pandemic.
Now that there is a widespread loss of trust in our longstanding epistemological system (science), two separate issues have emerged:
•The medical industry is suffering from a loss of public trust in many products that previously could be easily sold without scrutiny (e.g., vaccines).
•A general trust in our scientific institutions is necessary for the smooth operation of society (e.g., while corrupt, the medical system also provides many vital and essential services).
As such, a political force has emerged which can create real reforms that will significantly improve the medical system. This, in turn, is a key reason why RFK was able to get the otherwise almost improbable H.H.S. Secretary nomination, and why the “highly controversial” figure Jay Bhattacharya became the NIH director.
Since becoming the NIH director, Bhattacharya has begun doing something rather unprecedented to restore public trust in science—going onto independent media platforms to speak candidly about the problematic state of science and how he will make the NIH (the premier institution for scientific research) fix this mess. For example, in an interview earlier this month, he explained why the mRNA platform had serious issues that made it inappropriate for public health and hence was being paused (whereas in contrast, the NIH had previously spent years investing a lot of money into the technology).
Note: in his Huberman interview, Bhattacharya also discussed how the mRNA vaccines were not sufficiently tested, that public health authorities repeatedly claimed they could do things the data did not show, and that their side effects needed to be studied rather than censored.
Having watched these interviews, I find it incredible to see an NIH director openly critique the major shortcomings within science, rather than simply tell us how wonderful science is and that we must all trust the experts (which is what virtually every federal health official has always said). Of them, the two most noteworthy were:
The first was a recent (shorter) one with Alex Berenson earlier this month (which can be listened to on his Substack here).
The second was a longer June one with Andrew Huberman:
The New NIH
Throughout these interviews, Bhattacharya repeatedly pledged for greater transparency (which thus far he has done) and highlighted the steps he plans to take to restore trust in science.
One of the lessons I’ve learned during the pandemic…the mistake I saw over and over again was this desire to use science communications to manipulate the public, to vastly underestimate the capacity of the public to understand nuance, and oversimplify and demonize who disagreed with the public health message as if they were somehow the enemy.
I think all of those things breed distrust, it miseducates the public about what science is learning and discovering and what it is not learning and discovering, and if it impinges on people’s lives in ways that end up hurting them (like their children can’t go to school for years and they’re depressed or they’re addicted to opioids after their doctors and everyone are telling them that these things can’t get your addicted, they’re fired from their job on the premise COVID stops you from spreading COVID). All of these things are the fruits of a paradigm that views scientific communication as something which ought to lord over you rather than something which helps you decide how to make good decisions about your life.
Note: this is very similar to the core issues surrounding the public debate over if it was appropriate to use propaganda on the American people roughly a century ago (where sadly the propagandists eventually won—something I believe was extremely damaging to our society).
Essentially, we created a class of unclean people as a matter of public policy. You can understand why people who went through that would say, ‘Given that the vaccine didn’t turn out to stop you from getting and spreading COVID, why should I trust you on anything else?’ That, that’s where we currently are.
Scientific Epistemology
First, Bhattacharya shares many of my views on epistemology and believes public trust in science can only be rebuilt if a robust epistemological framework underlies it which includes the following:
•The culture of science shifting to one where scientists become more humble, admit what they don’t know, and are comfortable (or even embrace) losing their “authority” if a position they had previously espoused proves to be wrong (rather than the existing paradigm where they attack those who try to prove or disprove their findings as a “threat to science”)—leading to many being reluctant to do so. I hence found it noteworthy Bhattacharya shared that he liked being proven wrong (a trait I share as discovering my errors often allows me to get closer to the deeper truths I continually seek).
Note: science being “falsifiable” is often used by orthodox scientists to distinguish their science from (unorthodox) “pseudoscience.” Unfortunately, in many cases, orthodox (and “credible”) beliefs are often unfalsifiable and frequently not even permissible to publicly challenge.
•Bhattacharya believes science now in a very similar situation to where it was at in the 1700s immediately prior to the Enlightenment as relatively few authorities (specific “experts” and top journal editors) have the ability to decide what is true and are very hostile to anyone who questions their pronouncements. As such, we must shift the trust in scientific data from what anointed experts pronounce about existing datasets to it resulting from numerous authors successfully replicating existing published data (something which is necessary but rarely done).

Note: due to how many methods exist for doctoring studies, and the Academic press’s bias towards publishing new “exciting” findings, around half of studies cannot be replicated (with those failing replication actually being the most likely to be cited). This fact is an existential threat to science (and directly undermines both the trust we put in it and the justification for all the money we spend on it)—but until now, nothing has ever been done to address it.
To facilitate this, Bhattacharya is enacting a series of NIH policies (e.g., grants, tenure guarantees, and a high likelihood of a journal publication for replication studies) to incentivize researchers to engage in careers that conduct these vital replication studies (e.g., by making a NIH journal for publishing replication studies, making AI summaries prioritize replication efforts over Wikipedia articles, and having AI tool show what successful or unsuccessful replication attempts have been made on published studies). Likewise, he wants to crowd source ideas for the which widely cited studies are the most critical to attempt to replicate.
Note: Bhattacharya also wants to incentivize the publication of unsuccessful research, since as much, if not more, can be learned through studies which failed replication (and prevent unnecessary research from being conducted).
Free Speech
Bhattacharya repeatedly shared his experiences of being censored throughout COVID-19 (and people claiming he said the opposite of what he actually did) as a reason for why he feels it’s critical for him to defend free speech in science.
[T]he problem here is that the scientific community embraced an ethical norm about unity of messaging and then enforced it on fellow scientists. And then it cooperated with the Biden administration to put in place a censorship regime that made it impossible even for legitimate conversations [e.g., about vaccine injuries] to happen.
Note: during COVID, I saw many experts who previously had fairly reasonable views that used to be “moderate” and “non-controversial” become “far-right extremists” because they did not want to go along with the COVID lockdown mRNA push. In Bhattacharya’s case, most of his positions have been extremely reasonable ones that should not be controversial, but now are because there is so little room to have honest commentary in science that challenges existing dogmas.
There was essentially a groupthink at scale. It was impossible to organize a panel with the kind of diversity of opinion that was needed.
There were [a] million or more — I know this from the set of people who signed the Great Barrington Declaration, tens of thousands of scientists and doctors who disagreed [with the lockdowns], but they were afraid to stick their head up for fear of getting chopped off. It’s not an accident that Stanford didn’t allow a scientific panel with my point of view about the efficacy of lockdowns until 2024.
During COVID, because he broke from the narrative (e.g., on lockdowns or COVID being a lab leak), Bhattacharya was repeatedly attacked and censored. For example:
Yet those [Stanford professors] speaking out against Bhattacharya and Atlas’ views say they are doing so to fight misinformation that could have dangerous consequences.
The University has suggested that the issue at hand is simply a ‘difference of opinion,’ … or the academic freedom to express one’s personal views,” David Relman, a medicine, microbiology and immunology professor, wrote in an email to The Daily. “This is wrong; this is not the issue. This is not a difference of opinion about policy. It is a long series of flat-out lies about science.
Note: Bhattacharya thought this was quite extraordinary, as the press decided unless you had an epidemiology and virology background you could not comment on COVID-19, yet despite having both of these (along with an even more important health economics background) he still was cancelled due to him not supporting the narrative.
Overtrusting Experts
I feel as the director if I weigh in on a topic, I want to be listened to based on my reading of the evidence rather than my authority as head of NIH.
One of the key points Bhattacharya emphasizes is that scientific experts can no longer receive the same unconditional trust they used to (and rather that our trust must shift to being in impartial replication).
Note: Bhattacharya also mentions that Eisenhower warned against scientific aristocrats in his famous farewell address and that due to the miracles science has created, our culture is vulnerable to a deification of scientists (e.g., many worshipped Fauci and he appeared to crave it, which Berenson’s highlighted by noting he kept “I love you Fauci” letters on his office wall).
Another is that many public health scientists have allowed them to delude themselves into believing their expertise in certain areas makes them qualified to make consequential decisions about subjects far outside their expertise like running society (something many have also noticed is a common issue with doctors [and termed ultracrepidarianism]).
COVID, in turn, highlighted this issue, as decisions like lockdowns involved far more than a simply calculus of “stopping the spread” and since these other issues weren’t taken into consideration, it resulted in decisions (which caused far more harm than help) being forced upon us.
As such, Bhattacharya wants to have a far broader range of expertise be allowed into the conversation when deciding far-reaching scientific policies and likewise, to create a culture where scientists and labs collaborate with each other to determine scientific truth rather than everyone working independently (and prioritizing career advancement over scientific truth). Likewise, he want to create metrics for scientific achievement besides your number of publications and citations of your work such as “do you share data to allow replication attempts” or “do you answer questions in good faith”), as currently the incentives encourage hiding all of that.
Finally, Bhattacharya has highlighted some of the NIH’s gross failures (e.g., it exists to advance America’s health and longevity, yet from 2012-2019 there was almost no improvement in life expectancy and people now spend the last decade or more of their live’s sick) to illustrate why the current “trust in experts” has been an incredible waste of national resources.
Note: there are many other examples of the abuse of NIH research money by a corrupt system which others have discussed (e.g., RFK Jr. has mentioned how our massive Alzheimer’s research budget was squandered on scientific fraud).
Other Initatives
Bhattacharya also shared a variety of other initiatives he wanted implemented. These included:
• Having an open dialog with the public about what NIH was actually doing (both to increase public engagement with science and create public trust).
• Making all NIH-funded research be free for public consumption rather than behind journal paywalls.
• Engaging in important research the public wants but the scientific community has been unwilling to conduct (e.g., do vaccines cause autism) and conducting the research in an open source manner (e.g., holding public competitions to see who should get grants to conduct research).
• Focus on prioritizing quality science which advances America such as by investing in and training young scientists (as they typically produce the most paradigm shifting work) and to balance grants between basic and applied research.
• Reforming the funding institutions can siphon from grants to prevent the academic talent and research from being concentrated at coastal universities.
Note: I believe another key step for Bhattacharya to take is to reform the process for how Pubmed indexes journals so more controversial studies can enter the system and “exist” to the mainstream scientific community.
Conclusion
Many throughout history have observed that societies and their institutions follow a similar pattern:

Presently, Western science and medicine are considered to be the “best in the world” and I believe that this lack of accountability has caused these professions to shift from focusing on producing the results which earned them their credibility to dogmatic institutions more concerned about retaining their power, prestige and funding rather than producing results. As such, I would argue what we are witnessing with the MAHA revolution in government and the NIH illustrates an inevitable historical cycle playing out.
However, exactly how fast it takes things to go upwards is anything but set in stone as what Bhattacharya (and RFK) are setting out to do with the NIH and science many is analogous to cleaning the Augean stables (one of the “impossible” labors Hercules was given).
This is important because beyond us directly suffering for the rigid dogmatism of science, as Western science fails to deliver, it will be displaced (particularly since so much of the faith surrounding it was lost during COVID and the profession still has not apologized for its conduct).
For example, Bhattacharya highlighted how the US is now entering a period of separation and competition with China’s biomedical sector, where we risk either becoming siloed from them (and valuable discoveries that could advance humanity being lost) or being displaced by them.
Note: on this point Bhattacharya cited the siloing what happened during the U.S.S.R. (which produced a significant amount of valuable research almost no one knows about that I periodically reference here).
Likewise, more and more, the algorithmic (and close-minded) style of thinking doctors are trained in is being superseded by AI, and my strong suspicion is that if doctors cannot move beyond that, they will be rapidly displaced by AI. For example:
•AI systems are now greatly exceeding human performance on licensing examinations (this is not surprising).
•A recent study found that experienced doctors who used ChatGPT rather than standard electronic references were more accurate in their diagnoses (76% vs. 74%), but when ChatGPT alone was used, diagnostic accuracy was 92%.
•Patients are frequently discovering AI is more helpful to them than their doctors.
All of this in turn says to me that there is now an extraordinary confluence of factors (e.g., public interest, favorable H.H.S. leadership, and economic pressure on the medical system) that can allow the previously unchangeable scientific apparatus to start addressing critical scientific topics which affect all of us. At the start of this article I highlighted the chronology of the Yale LISTEN study (and the relentless censorship it has faced for simply trying to lay the foundation for acknowledging vaccine injuries exist) to show why the existing science paradigm is failing and beyond desperately needing reform, its gradually becoming unsustainable.
However, exactly how long it will be before things can move in a positive direction is highly dependent on the public support we can give the current attempts by MAHA to reform this mess. For that reason, beyond publicly voicing our objections to things we do not like, it is vital we also support and magnify efforts like those by Bhattacharya to fix things. I believe we can, and I am grateful to each of your who has helped make this shift possible.
An index of all the articles published in the Forgotten Side of Medicine (including each DMSO article) can be viewed here. Additionally, to learn how other readers have benefitted from this publication and the community it has created, their testimonials can be viewed here.
Click this link for the original source of this article.
Author: A Midwestern Doctor
This content is courtesy of, and owned and copyrighted by, https://amidwesterndoctor.substack.com and its author. This content is made available by use of the public RSS feed offered by the host site and is used for educational purposes only. If you are the author or represent the host site and would like this content removed now and in the future, please contact USSANews.com using the email address in the Contact page found in the website menu.



