
Dear Dr. Prasad,
I am grateful that the recent HHS publication of “COVID Recommendation FAQ” states:
“…the CDC will no longer recommend the COVID-19 vaccine for healthy children or pregnant women. In addition, after two years on the market, the safety and efficacy of the vaccines for healthy children younger than 12 or pregnant mothers has not been established by the manufacturers. There is also information from the COVID-19 manufacturers, FDA, and CDC, detailing serious adverse effects for children between 12 and 17 years of age.” https://www.npr.org/2025/06/13/nx-s1-5431935/rfk-hhs-covid-vaccine-schedule-faq

Yet I question the following recommendation: “The COVID-19 vaccine will only be recommended for children and pregnant women who are immunocompromised…”:
- Has the safety and efficacy of the covid ‘vaccines’ in immunocompromised children and pregnant women been established with well-controlled studies measuring severe clinical outcomes such as severe illness, hospitalization, or death?
- Are surrogate measures of vaccine-induced antibody titers being used as evidence supporting continued vaccination in immunocompromised children and pregnant women?
- If so, have covid vaccine-induced antibody titers been “validated” as a surrogate endpoint?
- Note: “Biomarkers and surrogate endpoints alone do not give us the total picture of benefit and risk of a therapy… These limitations underscore the importance of continued evaluation in the post-market phase when products are approved based upon surrogate endpoints that have not been validated, as well as the need to rigorously evaluate and sometimes re-evaluate surrogate endpoints clinically.”
https://www.cdc.gov/covid/hcp/clinical-care/overview-testing-sars-cov-2.html
https://www.fda.gov/about-fda/innovation-fda/fda-facts-biomarkers-and-surrogate-endpoints

Also, while the COVID Recommendation FAQ states “an increased risk of myocarditis and pericarditis… is highest in young males…,” the new (pending) safety warnings demonstrate “…the highest estimated incidence of myocarditis and/or pericarditis was in males 16 through 25 years of age.”
- What is the rationale for stopping the routine covid vaccine recommendation at age 17, but recommending it for young adults ³ 18 years old (the CDC states high risk of myocarditis and/or pericarditis up to age 39)?
https://www.fda.gov/media/186581/download?attachment
https://www.fda.gov/media/186580/download?attachment
Again, I am grateful for the evolving understanding of benefit-risk assessment of the covid vaccines.

Over three years ago, on January 19, 2022, I submitted a Citizen Petition to the FDA regarding protection of pregnant women and children under 45 CFR 46. For children, I had concluded that there was “greater than minimal risk” and “no prospect of direct benefit.”
https://www.regulations.gov/document/FDA-2022-P-0086-0002
On March 24, 2022, although my petition was denied in its entirety, there were aspects within the response significant today:
Request to Revoke EUAs and BLA Approvals for Pediatric Populations:
- “…advisory committees agreed that there is a serious risk of severe COVID-19 in pediatric populations.”
- “…FDA may revise or revoke an EUA if…a material change in the risk/benefit assessment based on evolving understanding of the disease or condition…may make an EUA unnecessary.”
Requests to Suspend Clinical Trials for All Pediatric and Pregnant
Subpopulations and to Add Exclusion Criteria for Pediatric and Pregnant Subpopulations:
- “FDA does not believe that human subjects in any ongoing COVID-19 vaccine clinical trial under IND including pediatric or pregnant subjects (including those that do not specifically exclude pregnant or pediatric individuals) are or would be exposed to an unreasonable and significant risk of illness or injury.” https://www.regulations.gov/document/FDA-2022-P-0086-0024
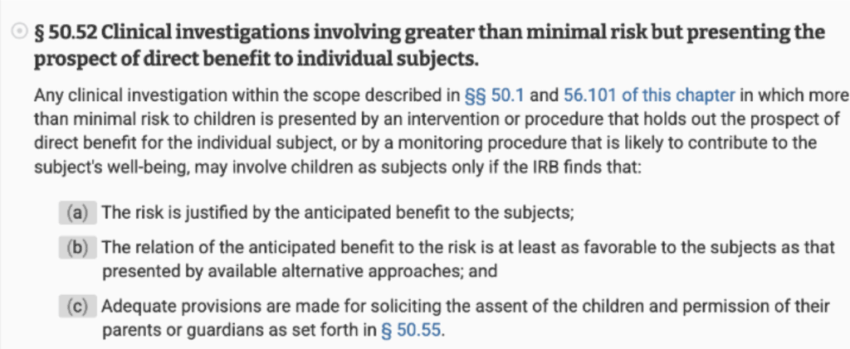
On July 20, 2022, Dr. Peter Marks confirmed the 45 CFR 46 risk category for children as “greater than minimal risk.” We differed in our opinion of “prospect of direct benefit”:
https://www.ecfr.gov/current/title-21/chapter-I/subchapter-A/part-50/subpart-D/section-50.52
“Research involving greater than minimal risk and no prospect of direct benefit” requires that “the risk represents [only] a minor increase over minimal risk” and that “[a]ny potential harms associated with the procedure will be transient and reversible in consideration of the nature of the harm (restricted to time of procedure or short post-experimental period).”
https://www.hhs.gov/ohrp/sachrp-committee/recommendations/2005-july-28-letter-appendix-b/index.html
HHS’s acknowledged benefit-risk profile of the covid vaccines today suggests that there would be “no prospect of direct benefit” and unjustifiable risk to healthy children and pregnant women within clinical trials.
Yet today, covid vaccine studies are still recruiting healthy children, such as the below, to include “participants” from the age of 6 months: https://www.clinicaltrials.gov/study/NCT05436834?term=moderna&aggFilters=ages:child,studyType:int&page=2&rank=11 – study-plan
As remarked by Secretary Kennedy, “Our infants and children deserve the best safety trials possible to keep them safe.” https://x.com/SecKennedy/status/1932580198198964241
So, lastly, I ask:
- Has “a material change in the risk/benefit assessment based on evolving understanding of the disease or condition…”:
- “make an EUA unnecessary” for children?
- preclude inclusion of pregnant women and children in covid vaccine trials due to “an unreasonable and significant risk of illness or injury”?
Dr. Prasad, I await your response to these critical questions.
Respectfully,
Carol Taccetta, MD, FCAP
The post “An Evolving Understanding of Benefit-Risk Assessment of the Covid ‘Vaccines’: Protecting Our Most Vulnerable” appeared first on DailyClout.
Click this link for the original source of this article.
Author: Sean Probber
This content is courtesy of, and owned and copyrighted by, https://dailyclout.io and its author. This content is made available by use of the public RSS feed offered by the host site and is used for educational purposes only. If you are the author or represent the host site and would like this content removed now and in the future, please contact USSANews.com using the email address in the Contact page found in the website menu.


