
Please Show Us the Trials
by Eyal Shahar at Brownstone Institute
In a recently published study, researchers from the Czech Republic report a rare, national-level analysis of Covid vaccines and all-cause mortality. Anyone with a critical mind should at least read the exemplary summary by Tomas Fürst on Brownstone and carefully study the figure.
Toward the end of the Brownstone article, Fürst writes:
“Yet, in the Mirror of Erised above, you can see that the vaccine may appear to be 80% effective, even against Covid-unrelated deaths! Still, we are not aware of any vaccine effectiveness studies that tried to correct for this huge HVE [healthy vaccinee effect, E.S.]. This means that all claims of Covid vaccine effectiveness since the beginning of the mass vaccination campaign must be revised. The vaccine’s true efficacy against death from Covid may have been zero, or even negative; we simply don’t know.”
I could not agree more. Repeated model-based claims about millions of saved life-years cannot be reconciled with simple mortality statistics—for example, a contrast of Israel with Sweden in the winter of 2020–2021 or elementary worldwide calculations. Having failed to penetrate the censorship machinery of biomedical journals, I devoted numerous posts to the healthy vaccinee bias and a method to remove it. However, just a few weeks after the Czech study was published, I finally published a peer-reviewed paper on the (corrected) effectiveness of a Covid vaccine. The road to publication was not easy. Even medRxiv refused to post a preprint on the basis of a ridiculous excuse. (“It is not a clinical research article with new data.”)
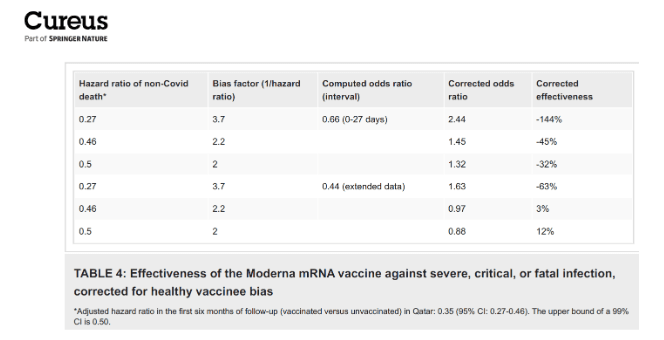
Using published data from Qatar, I was able to remove two key biases, one of which was the healthy vaccinee effect. The other bias, formally called immortal time, arose from excluding early events in the vaccinated, a common practice of vaccine effectiveness studies. Unfortunately, it is too technical to explain here. Removing that bias reduced estimates of effectiveness by a lot—sometimes from over 95 percent to less than 50 percent—and suggested early negative effectiveness.
As I explained in a book (chapter 37), the healthy vaccinee bias cannot be removed by an exact method, so we have two options: to accept the bias or to try to remove it by an imperfect method. In my paper, I justified and applied three correction factors to estimates of vaccine effectiveness. It is called sensitivity analysis. Under every correction, the effectiveness against a severe outcome of two early variants was negative in the first month and near zero, at best, by the time full immunity was reached. The original paper reported 100% effectiveness…
Immortal time and healthy vaccinee are not the only biases in observational studies of Covid vaccines. At least two more should be mentioned:
Vaccinated people were less likely to be tested for Covid than their unvaccinated counterparts, and therefore, they were less likely to be classified as cases of severe Covid and Covid deaths. In the taxonomy of biases, it is called information bias. We have unquestionable evidence that the bias was operating in Israel—“The Pfizer laboratory” —during the first vaccination campaign. This bias has probably affected studies from many countries.
Another source of bias was the timing of the vaccination campaigns, which often coincided with a Covid wave. As a result, the time-at-risk in an unvaccinated status was concentrated at the time of rising infection rates, whereas the time-at-risk in vaccinated status was concentrated at the phase of the decline. It is called confounding by time trends in the risk of the outcome. A few studies tried to prevent this bias by matching on calendar time; many did not.
A perfect storm of biases was operating at that time, and, as Fürst writes, “The true value of the vaccine effectiveness can only be derived from prospective randomized studies.”
I am wondering whether we will ever see them. Will the FDA continue to authorize new mRNA Covid vaccines each year solely based on their ability to generate antibodies? Might we be increasing the risk of an infection with more shots due to class switch to IgG4 antibodies? Should these shots continue to be administered to residents of nursing homes, if negative effectiveness is at least possible, and vaccine-related deaths have undoubtedly happened? Is it ethical to continue to approve a novel gene therapy without a single, well-designed, randomized trial with a mortality endpoint?
The FDA, under a new administration, has recently made progress in the right direction. I hope they will not stop there. Winter is too close for a trial this year, but there is plenty of time for the NIH to write up a Request for Applications for randomized trials next winter. The study population should be residents of nursing homes who can provide consent because that’s the high-risk population. Let’s see a comparison of next-year formulations of mRNA Covid vaccines with placebo, with a mortality endpoint: Covid deaths and all-cause deaths. Perhaps there should be a third arm for the flu shot.
Please Show Us the Trials
by Eyal Shahar at Brownstone Institute – Daily Economics, Policy, Public Health, Society
Author: Eyal Shahar
This content is courtesy of, and owned and copyrighted by, https://brownstone.org and its author. This content is made available by use of the public RSS feed offered by the host site and is used for educational purposes only. If you are the author or represent the host site and would like this content removed now and in the future, please contact USSANews.com using the email address in the Contact page found in the website menu.



