

‘Overall, the findings in this paper provided concerning evidence of a higher-than-expected fetal loss rate associated with mRNA COVID-19 vaccine doses received during early pregnancy (gestational weeks 8-13).
The safety signal should be further investigated by regulatory authorities as part of their risk assessment of vaccination during pregnancy with specific focus on the physiological effects in early pregnancy. There is also a need to conduct pathophysiological studies to better understand the potential biological mechanisms. Additionally, it would be insightful to assess the potential impact of non-mRNA COVID-19 vaccines. The findings also underscore the importance of conducting dedicated and statistically powered prospective clinical trials to study the impact of vaccination for COVID-19 and other pathogens during pregnancy to better inform recommendations to this vulnerable population.’
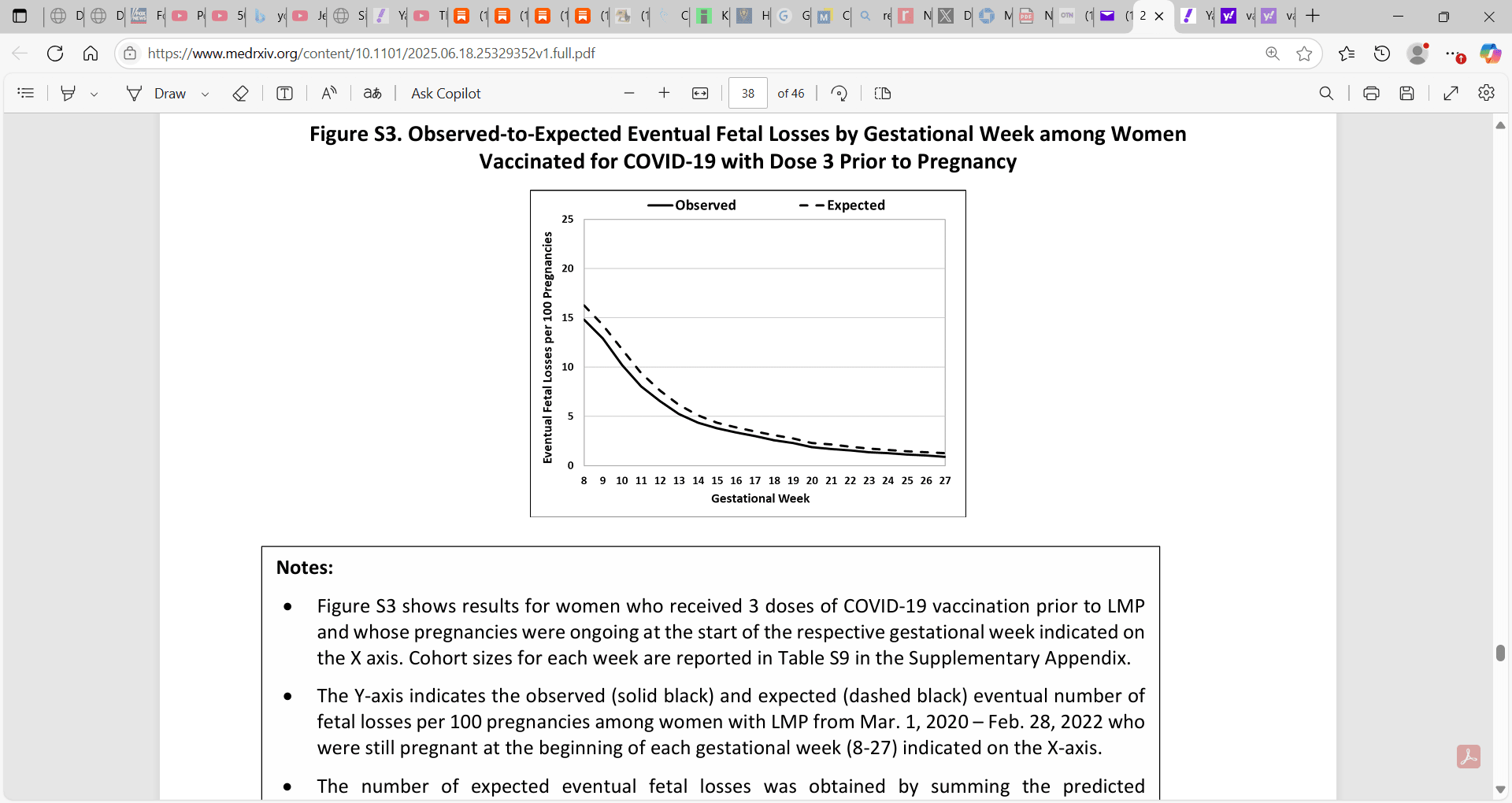
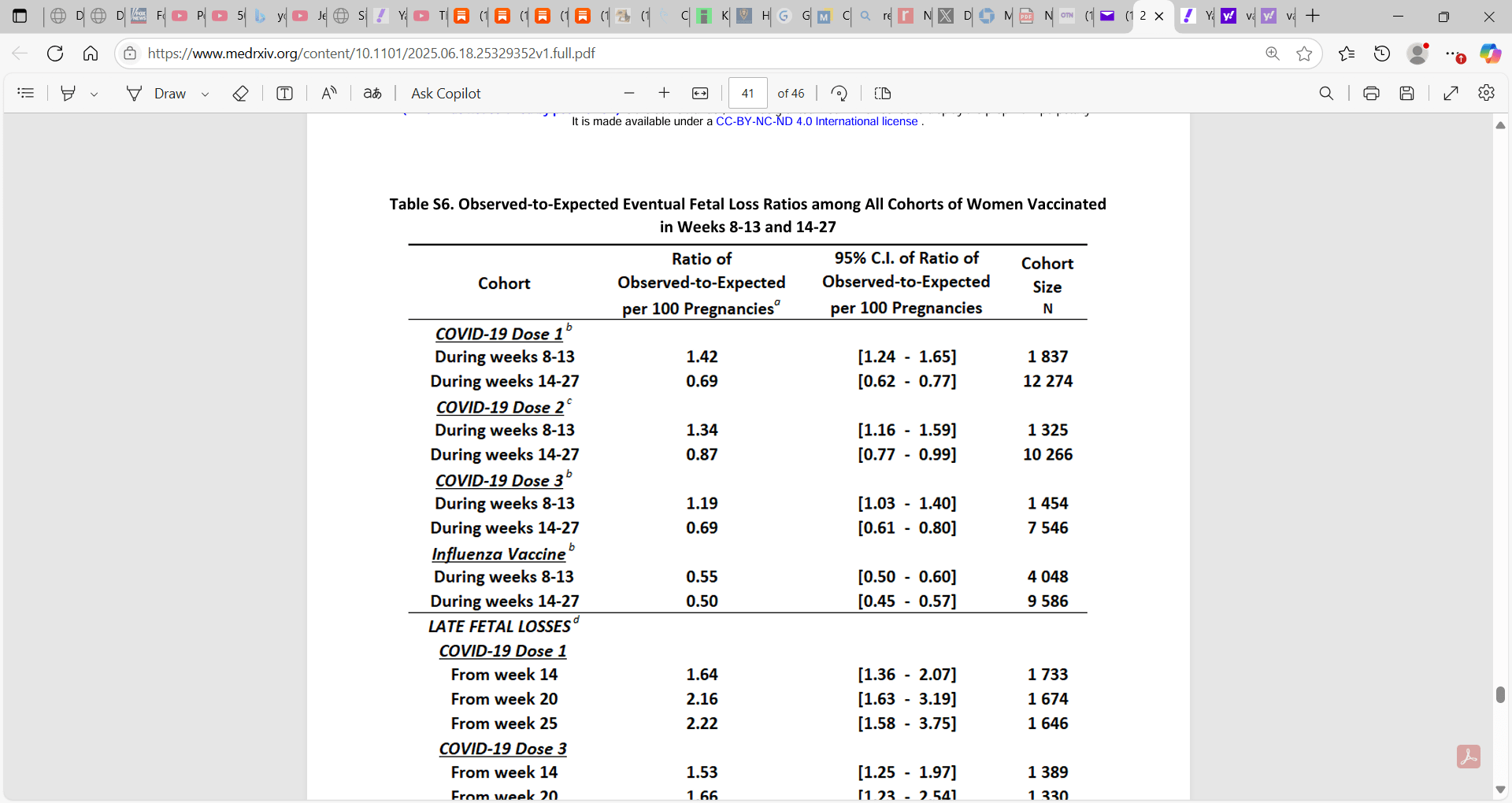
‘The results provide evidence for a substantially higher-than-expected number of eventual fetal losses associated with COVID-19 vaccination during gestational weeks 8-13.’
I ask you to please be cautious in any interpretation because as outlined below:
Alexander News Network (ANN): Trump’s War 2.0 for America is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.

1)as mentioned, the observed-to-expected analysis cannot be used to extrapolate to causality between Malone Bourla Bancel Moderna Pfizer et al. mRNA vaccine & elevated or decreased ‘fetal loss rates or quantify the magnitude of such potential impact.’
2)we have to be cognizant of unknown confounders (distorting confusing factors) that impact any definitive conclusions; such residual confounding is problematic in interpretation; researchers did clarify in this regard that ‘if there were, such unobserved confounders would have had to be unique to women who received vaccination for COVID-19 but not for influenza.’

‘They also would have needed to be relevant to women who vaccinated during gestational weeks 8-13 but not during weeks 14-27 or prior to pregnancy.’
Researchers also reminded us that ‘this study did not include gestational weeks 1-7 and therefore could not assess the potential impact of vaccination during that period.’
Researchers also explained (and I applaud them for this strong observational study, well done yet plagued with residual confounding and some methods constraints, yet sheer honesty recognizing the methodological issues e.g. a ‘general limitation of studies that are based on pregnancy registries stems from the fact that early fetal losses are often not documented, and more generally, the follow up may not be consistent across women.’ Moreover, ‘there were pregnancies in the registry that were excluded because of lack of appropriate and timely follow-up, and while the analysis did not point to any obvious related biases, it cannot rule them out.’
Researchers also state that ‘the Maccabi registry, like most pregnancy registries, did not provide sufficient information to distinguish between purely elective and medically-driven induced abortions. Thus, it is possible that some of the observed-to-expected differences are driven by behavioral mechanisms. For example, women who were vaccinated early in pregnancy may have been more likely to report fetal losses.’
Moreover, the researchers were correct to point out the issues of generalizability, extrapolation to other study groups or settings given the focus on Israeli data; ‘this study is based only on data from Israel, and it would be important to conduct studies with similar data from other countries to see whether the results replicate.’



‘The study includes pregnancies in Israel with last menstruation period (LMP) between March 1, 2016 and February 28, 2022. The main analysis presents observed-to-expected comparisons of the number of eventual fetal losses among pregnant women exposed to mRNA COVID-19 vaccination (almost all Pfizer) during gestational weeks 8-13 and 14-27, respectively.
Women vaccinated for influenza during gestational weeks 8-27, as well as women vaccinated prior to pregnancy for COVID-19 or influenza, were used as comparative controls. Cohort-specific expected number of fetal losses are established based on estimates from a regression model trained on historical data from 2016-2018 that incorporates individual-level risk factors and gestational week of each pregnant woman included in the cohort.
Results
Analysis of 226,395 singleton pregnancies in Israel from 2016 to 2022 indicates that COVID-19 vaccination with dose 1 during weeks 8-13 was associated with higher-than-expected observed number of fetal losses of approximately 13 versus 9 expected for every 100 exposed pregnancies, i.e., nearly 3.9 (95% CI: [2.55-5.14]) additional fetal losses above expected per 100 pregnancies Most of the excess fetal losses occurred after gestational week 20 and nearly half occurred after gestational week 25. Similarly, women vaccinated with dose 3 during weeks 8-13 exhibited a higher-than-expected number of fetal losses with nearly 1.9 (95% CI: 0.39-3.42]) additional fetal losses above expected per 100 pregnancies. In contrast, pregnant women vaccinated for influenza during weeks 8-27 exhibited a consistently lower-than-expected observed number of fetal losses, likely the result of healthy vaccinee bias. Women vaccinated for COVID-19 or influenza prior to pregnancy exhibited according-to-expected or lower-than-expected numbers of fetal losses.
Conclusion
The results provide evidence for a substantially higher-than-expected number of eventual fetal losses associated with COVID-19 vaccination during gestational weeks 8-13.’
2025.06.18.25329352v1.full.pdf








___
You must not wait for another catastrophic crisis (at times manufactured but we are prevented from making our own basic personal decisions or accessing needed drugs and response tools) to catch you off-guard. We must take charge and be prepared today so that we can enjoy peace of mind tomorrow.
Enter the Wellness Company as a solution and a willing participant in the health care conversation. The Wellness Company, launched in 2022, offers health care, prescriptions, and supplements, all backed by research
The Wellness Company isn’t chasing profits — it’s trying to help people recover. While the government continues pushing vaccines, The Wellness Company is focusing on real solutions.
From telemedicine, prescriptions, memberships, and supplements, TWC is leading America with alternative choices to the traditional health care model.
Please consider support of a good PATRIOT company (in this PATRIOT economy) Drs. McCullough, Risch, Thorp, myself support (they are our sponsors), The Wellness Company; see the emergency preparation kit (key component being antibiotics you were denied by doctors, pharmacists, governments during the fraud COVID), first aid kit, travel emergency kit, contagion control kit etc. Please consider the SPIKE SUPPORT (spike protein DETOX dissolving spike from mRNA vaccine, this is critical to remove spike form the mRNA vaccine/and DNA viral vector) formula with NATTOKINASE as well as the triple formula (SPIKE SUPPORT, BROMELAIN, CIRCUMIN)
If you wish to give a donation to help me, you can at:
Zelle:
Or Ko-Fi
Ko-fi.com/drpauleliasalexander
Or to my address at:
150 South 8th Street
Unit 170
Lewiston, New York
14092
Alternatively, please consider going from an UNPAID subscriber or follower to a PAID at $5 per month or $30 per year. This can provide me help. If this is not possible at this time, this is ok, please remain a subscriber for FREE and there is no difference between FREE and PAID. No restrictions.
Click this link for the original source of this article.
Author: Dr. Paul Alexander
This content is courtesy of, and owned and copyrighted by, https://palexander.substack.com and its author. This content is made available by use of the public RSS feed offered by the host site and is used for educational purposes only. If you are the author or represent the host site and would like this content removed now and in the future, please contact USSANews.com using the email address in the Contact page found in the website menu.



